Prosthetic restoration of the maxillary anterior teeth using implantation and forced eruption: Case report
- Affiliations
-
- 1Department of Dentistry, Collage of Medicine, Soon Chun Hyang University, Cheonan, Korea. kyoungkyu@hanmail.net
- KMID: 2000287
- DOI: http://doi.org/10.4047/jkap.2011.49.1.80
Abstract
- When a tooth adjacent to implant has coronal damages caused by severe dental caries or fracture, the clinical crown lengthening by forced eruption makes it possible to get esthetic restoration due to the prevention of alveolar crestal bone resorption and loss of interdental papilla. A 54-years-old male patient wanted prosthetic treatment because his anterior 3 unit bridges had fallen out. A right maxillary central incisor showed mild dental caries but a right maxillary canine lost most clinical crowns. Forced eruption combined with a gingival fiberotomy of a right maxillary canine was performed for 1 month after the dental implant had been simultaneously placed with bone grafts on a right maxillary lateral incisor. About 5 months after implant placement, 2nd surgical operation was performed. The provisional restorations were adjusted to make esthetic gingival contour for 8 weeks. The porcelain fused gold restorations were fabricated and set. The patient was satisfied with the final restorations in esthetic and functional aspect.
Keyword
MeSH Terms
Figure
-
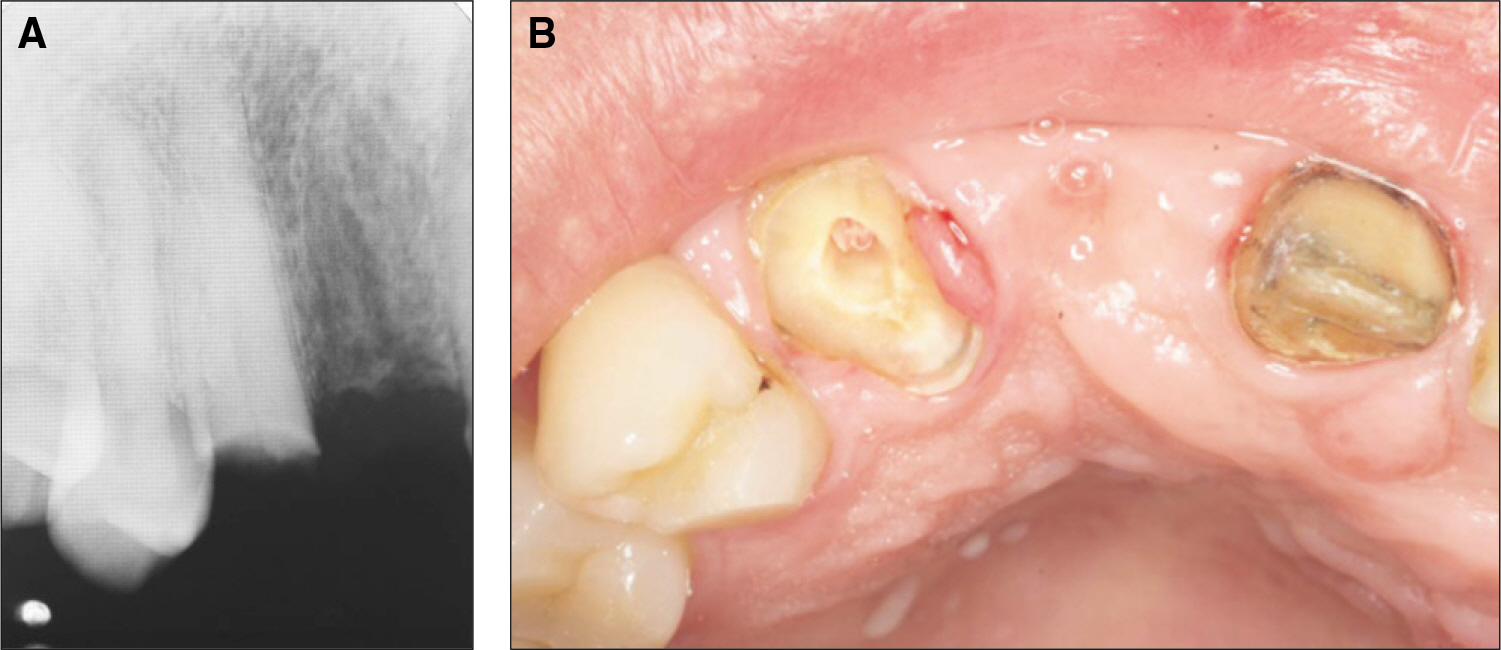
Fig. 1. Periapical radiograph and intraoral photo at first visit. A: The maxillary right canine was fractured, B: Intraoral view after caries removal and endodontic treatment of the maxillary right canine.
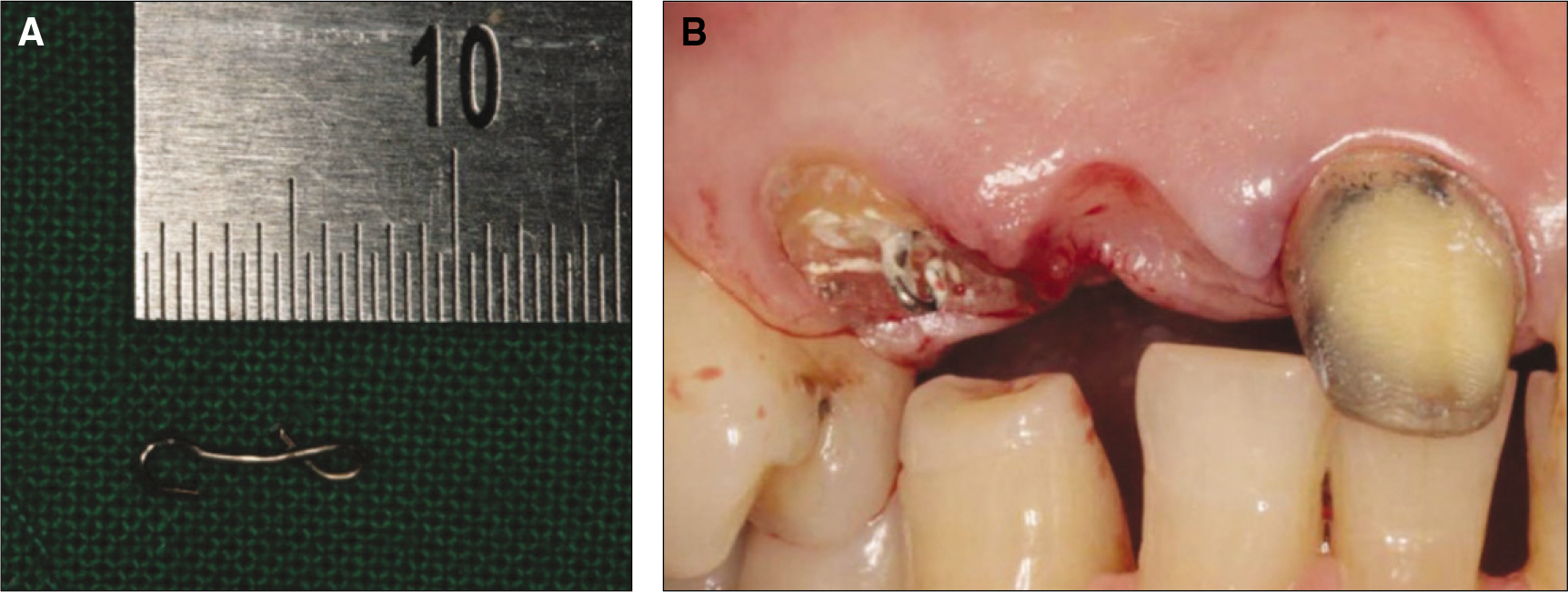
Fig. 2. Cementation of a temporary post with hook A: A temporary post with hook, B: A temporary post with hook was cemented into the retained root.
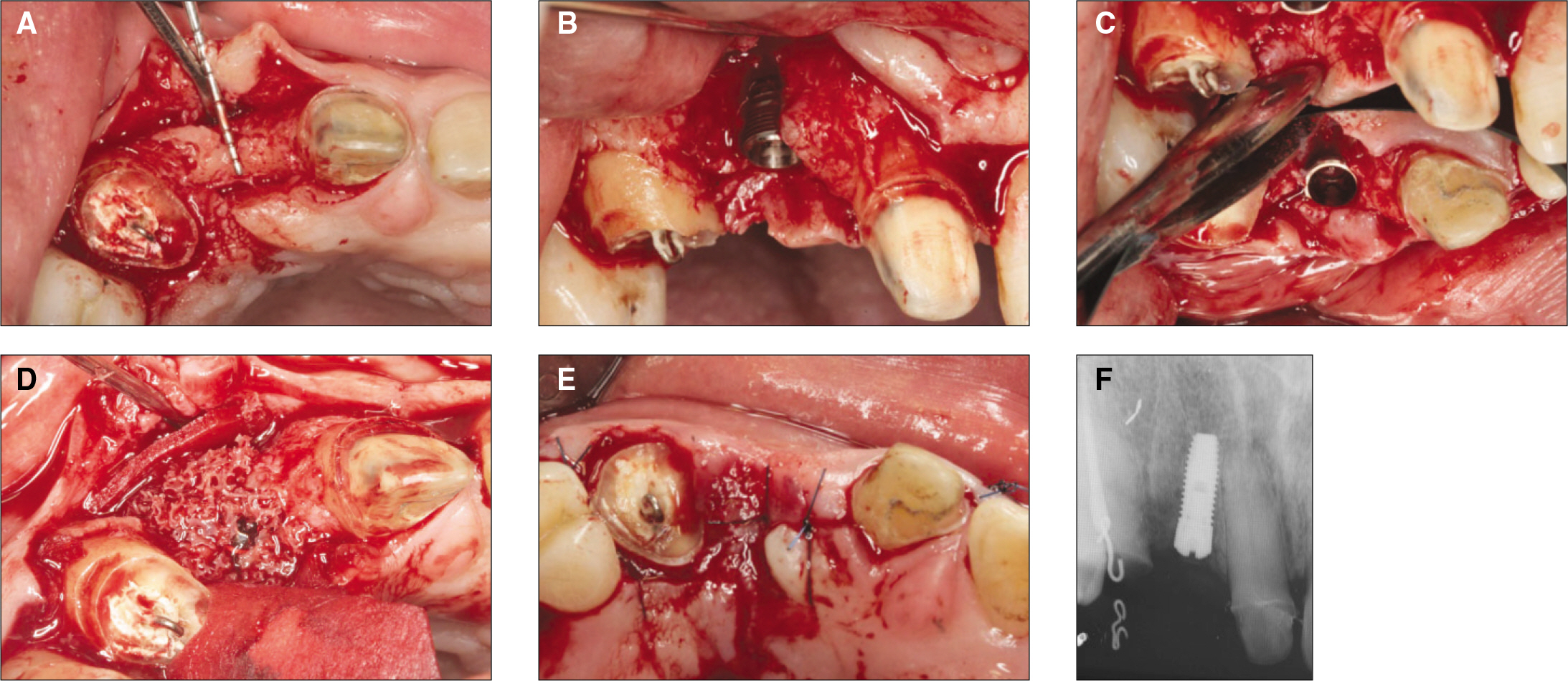
Fig. 3. Implantation of the maxillary right lateral incisor. A: Occlusal view: Note the narrow alveolar ridge, B: Buccal dehiscence following implant placement, C: Palatal dehiscence following implant placement, D: GBR with ICB and lyoplant membrane, E: Primary closure was attained, F: Postoperative periapical radiograph.
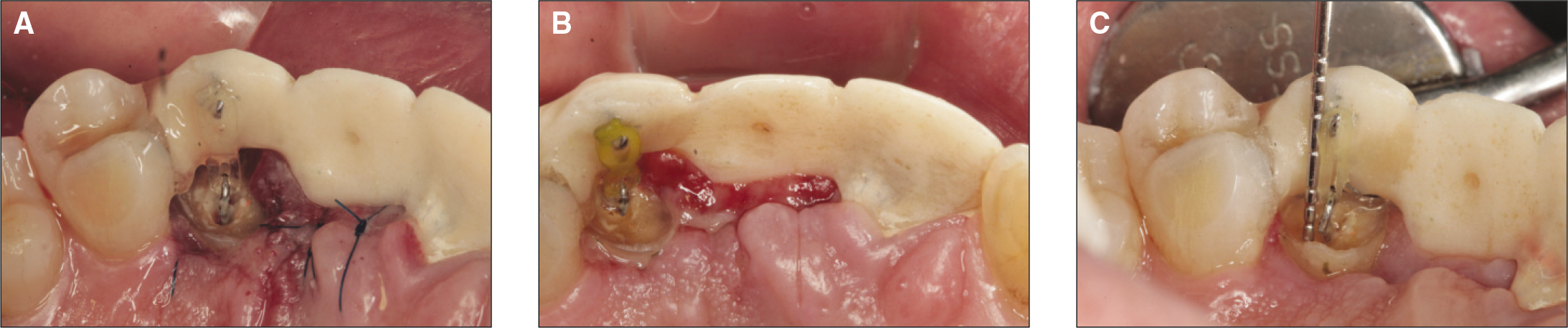
Fig. 4. Forced eruption. A power chain placed between the hook on the retained root and the hook on the provision. A: First day, B: after 1week, C: after 3 weeks.

Fig. 5. The provisional restorations were repeatedly adjusted to control the contour of the marginal gingiva and the interdental papilla for 8 weeks.

Fig. 6. Final impression with temporary custom abutment.

Fig. 7. Metal cap try in.
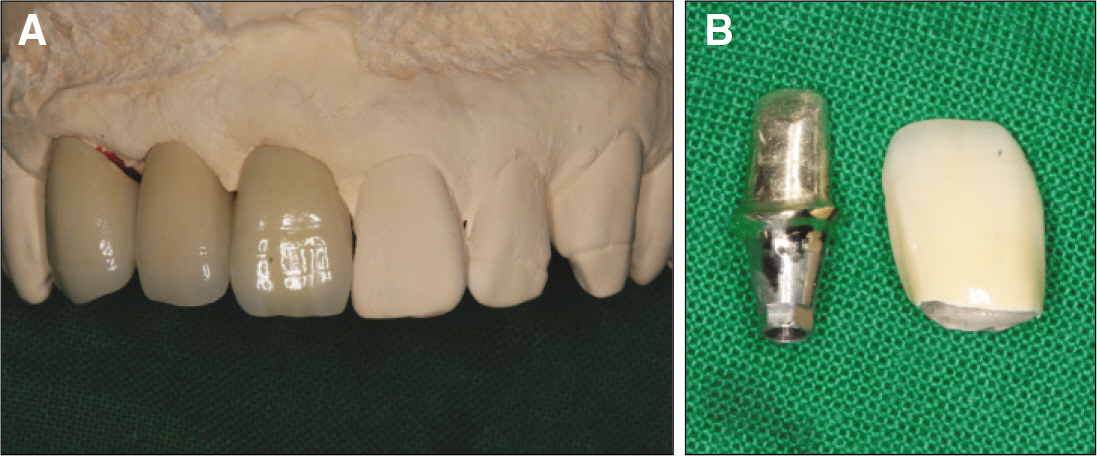
Fig. 8. Final restorations in working cast. A: working cast, B: Customized gold casting abutment and porcelain fused to gold crown.
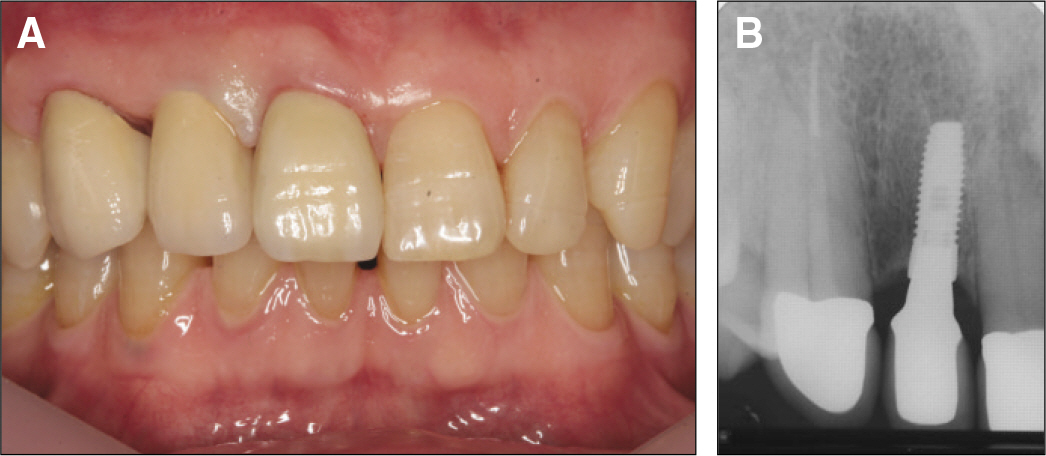
Fig. 9. The final restorations. A: PFG crowns were set, B: Radiograph after the insertion of the PFG crowns.
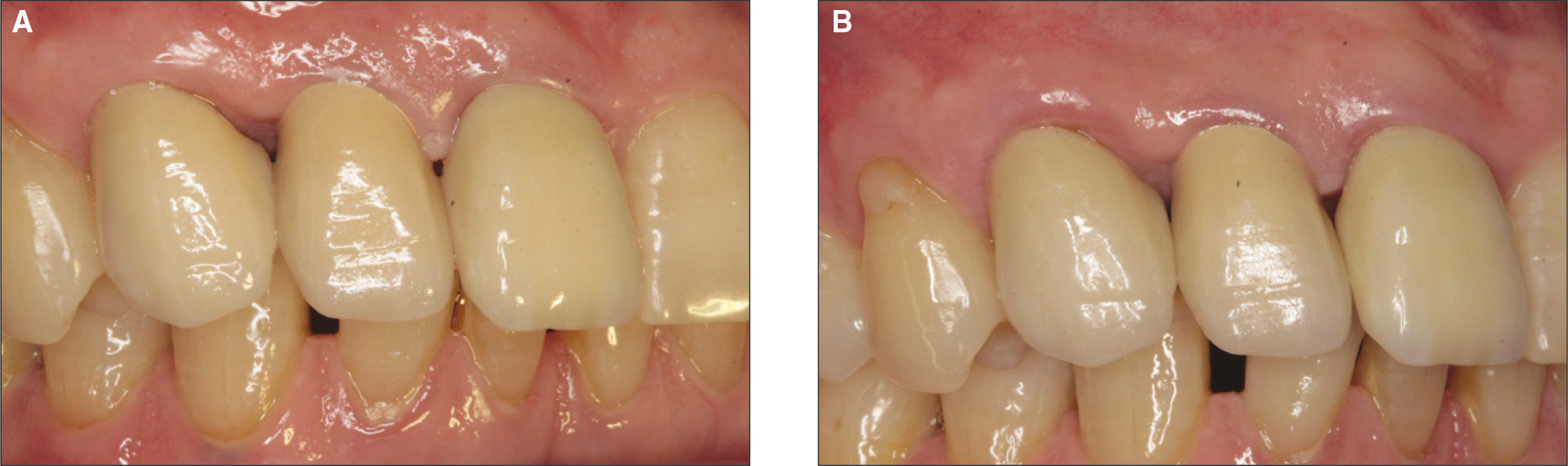
Fig. 10. follow up check. Inter-dental papilla of canine and lateral incisor was gradually filled. A: Photo taken 3 months after final cementaion, B: Photo taken 6 months after final cementation.
Cited by 1 articles
-
Esthetic restoration of subgingival crown-root fractured maxillary anterior tooth using surgical extrusion
So-Jin Lee, Yu-Jin Kim, Young-Bum Park, Kyoo-Sung Cho, Moon-Kyu Chung
J Korean Acad Prosthodont. 2012;50(3):204-209. doi: 10.4047/jkap.2012.50.3.204.
Reference
-
1.Choquet V., Hermans M., Adriaenssens P., Daelemans P., Tarnow DP., Malevez C. Clinical and radiographic evaluation of the papilla level adjacent to single tooth dental implants. A retrospective study in the maxillary anterior region. J Periodontol. 2001. 72:1364–71.2.Tarnow DP., Magner AW., Fletcher P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J Periodontol. 1992. 63:995–6.
Article3.Elian N., Jalbout ZN., Cho SC., Froum S., Tarnow DP. Realities and limitations in the management of the interdental papilla between implants: three case reports. Pract Proced Aesthet Dent. 2003. 15:737–44.4.Tarnow D., Elian N., Fletcher P., Froum S., Magner A., Cho SC., Salama M., Salama H., Garber DA. Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J Periodontol. 2003. 74:1785–8.
Article5.Assif D., Pilo R., Marshak B. Restoring teeth following crown lengthening procedures. J Prosthet Dent. 1991. 65:62–4.
Article6.Ingber JS. Forced eruption. I. A method of treating isolated one and two wall infrabony osseous defects-rationale and case report. J Periodontol. 1974. 45:199–206.7.Kozlovsky A., Tal H., Lieberman M. Forced eruption combined with gingival fiberotomy. A technique for clinical crown lengthening. J Clin Periodontol. 1988. 15:534–8.
Article8.Pontoriero R., Celenza F Jr., Ricci G., Carnevale G. Rapid extrusion with fiber resection: a combined orthodontic-periodontic treatment modality. Int J Periodontics Restorative Dent. 1987. 7:30–43.9.Funato A., Salama MA., Ishikawa T., Garber DA., Salama H. Timing, positioning, and sequential staging in esthetic implant therapy: a four-dimensional perspective. Int J Periodontics Restorative Dent. 2007. 27:313–23.10.Edwards JG. Soft-tissue surgery to alleviate orthodontic relapse. Dent Clin North Am. 1993. 37:205–25.11.Kinsel RP., Capoferri D. A simplified method to develop optimal gingival contours for the single implant-supported, metal-ceramic crown in the aesthetic zone. Pract Proced Aesthet Dent. 2008. 20:231–6.12.Soadoun AP., Touati B. Soft tissue recession around implants: is it still unavoidable?-Part II. Pract Proced Aesthet Dent. 2007. 19:81–7.13.Small PN., Tarnow DP. Gingival recession around implants: a 1-year longitudinal prospective study. Int J Oral Maxillofac Implants. 2000. 15:527–32.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Conservative approach for anterior crown-root fractured teeth: forced eruption
- Decoronation and implant restoration of ankylosed tooth resulted from anterior avulsion: A case report
- Stepwise fixed prosthetic restoration using facial scan in skeletal class II malocclusion patient: a case report
- Effect of slow forced eruption on the vertical levels of the interproximal bone and papilla and the width of the alveolar ridge
- Esthetic enhancement of a traumatized anterior tooth with a combination of forced eruption and tooth alignment: a case report
