J Korean Acad Prosthodont.
2012 Jul;50(3):210-215. 10.4047/jkap.2012.50.3.210.
Oral rehabilitation of a young adult with amelogenesis imperfect using metal-ceramic restoration: a clinical report
- Affiliations
-
- 1Department of Prosthodontics, College of Dentistry, Yonsei University, Seoul, Korea. hwm5@yuhs.ac
- KMID: 2000211
- DOI: http://doi.org/10.4047/jkap.2012.50.3.210
Abstract
- Some patients with generalized attrition and teeth discoloration may want their anterior teeth to be treated just for esthetic improvement. Ameologenesis imperfecta, however, should be considered for such patients prior to any treatment with thorough clinical and radiographic examination. If a patient is diagnosed with amelogenesis imperfecta, the treatment on anterior teeth just for esthetic purpose is not advisable. In this case, a young man with amelogenesis imperfecta was treated with metal-ceramic restorations. The patient had generalized attrition, teeth discoloration, crown fracture, and cross-bite on the left teeth. The ultimate objective of this treatment was to enhance esthetics and masticatory function. The cross-bite on the left anterior teeth was treated with restorations, whereas the reverse horizontal overlap was maintained on the posterior. The patient was satisfied with the result esthetically and functionally, and the third month recall examination revealed no pathologic changes associated with the treatment.
Figure
-

Fig. 1 Initial intraoral view.

Fig. 2 Initial panoramic radiograph.
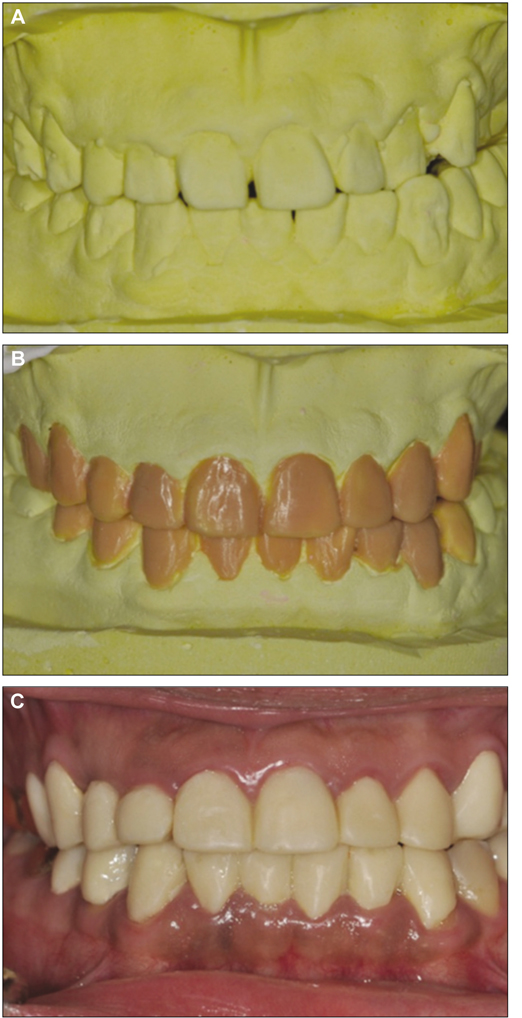
Fig. 3 A: Initial preliminary cast, B: diagnostic wax-up, and C: provisional restoration.

Fig. 4 Intraoral view of final prosthesis.
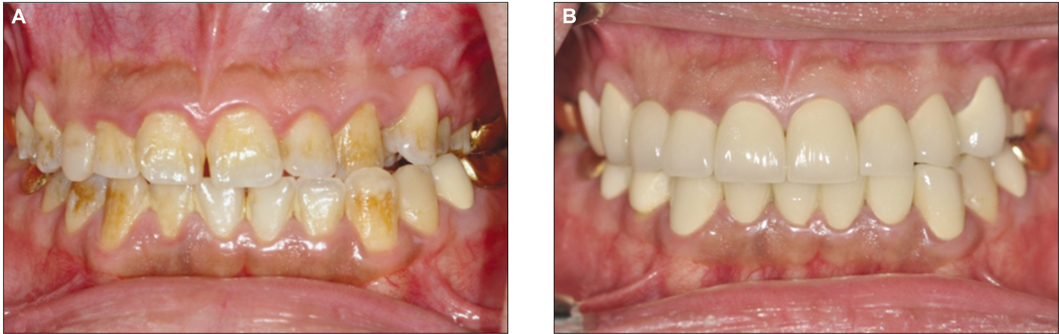
Fig. 5 Intraoral photos A: at first visit and B: after the placement of prosthesis.
Reference
-
1. Rao S, Witkop CJ Jr. Inherited defects in tooth structure. Birth Defects Orig Artic Ser. 1971. 7:153–184.2. Aldred MJ, Savarirayan R, Crawford PJ. Amelogenesis imperfecta: a classification and catalogue for the 21st century. Oral Dis. 2003. 9:19–23.
Article3. Sundell S, Valentin J. Hereditary aspects and classification of hereditary amelogenesis imperfecta. Community Dent Oral Epidemiol. 1986. 14:211–216.
Article4. Witkop CJ Jr. Amelogenesis imperfecta, dentinogenesis imperfecta and dentin dysplasia revisited: problems in classification. J Oral Pathol. 1988. 17:547–553.
Article5. Aldred MJ, Crawford PJ. Variable expression in Amelogenesis imperfecta with taurodontism. J Oral Pathol. 1988. 17:327–333.
Article6. Seow WK. Clinical diagnosis and management strategies of amelogenesis imperfectavariants. Pediatr Dent. 1993. 15:384–393.7. Coffield KD, Phillips C, Brady M, Roberts MW, Strauss RP, Wright JT. The psychosocial impact of developmental dental defects in people with hereditary amelogenesis imperfecta. J Am Dent Assoc. 2005. 136:620–630.
Article8. Yip HK, Smales RJ. Oral rehabilitation of young adults with amelogenesis imperfecta. Int J Prosthodont. 2003. 16:345–349.9. Bharath Shetty Y, Shetty A. Oral rehabilitation of a young adult with amelogenesis imperfecta: a clinical report. J Indian Prosthodont Soc. 2010. 10:240–245.
Article10. Oliveira IK, Fonseca Jde F, do Amaral FL, Pecorari VG, Basting RT, França FM. Diagnosis and esthetic functional rehabilitation of a patient with amelogenesis imperfecta. Quintessence Int. 2011. 42:463–469.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fabrication of a metal-ceramic crown to fit an existing partial removable dental prosthesis using ceramic pressed to metal technique: a clinical report
- Full-mouth rehabilitation in an amelogenesis imperfecta patient with anterior open bite using CAD/CAM system
- Fabricating a Ceramic-Pressed-to-Metal Restoration with Computer-Aided Design, Computer-Aided Manufacturing and Selective Laser Sintering: A Case Report
- Comparative study in marginal fit of a pressed ceramic and feldspathic porcelain fused to metal restoration
- The effect of improperly contoured and poor fitting restorations to patient with oral lichen planus: periodontal and prosthetic treatment
