Palatal obturator restoration of a cleft palate patient with velopharyngeal insufficiency: a clinical report
- Affiliations
-
- 1Department of Prosthodontics, College of Dentistry, Chosun University, Gwangju, Korea. jhajung@chosun.ac.kr
- KMID: 2000161
- DOI: http://doi.org/10.4047/jkap.2013.51.4.353
Abstract
- Cleft lip and palate is congenital deformity in oral and maxillofacial area. Normal soft palate has velopharyngeal closure action by connecting oral cavity and nasal cavity at rest and moving upward at swallowing and specific pronunciation. Cleft palate patients with velopharyngeal insufficiency have difficulty in mastication, swallowing and pronunciation because velopharyngeal closure is incomplete. At this time, a prosthetic device used to cover palate defects is called a palatal obturator. A palatal obturator separates oral cavity and nasal cavity and recovers pronunciation, mastication, swallowing and esthetic function. The purpose of this case study is to report the results because it reaches a satisfactory result in functional and esthetic aspects through functional impression procedures using modeling compound and tissue conditioner for restoration of a cleft palate patient with velopharyngeal insufficiency.
MeSH Terms
Figure
-
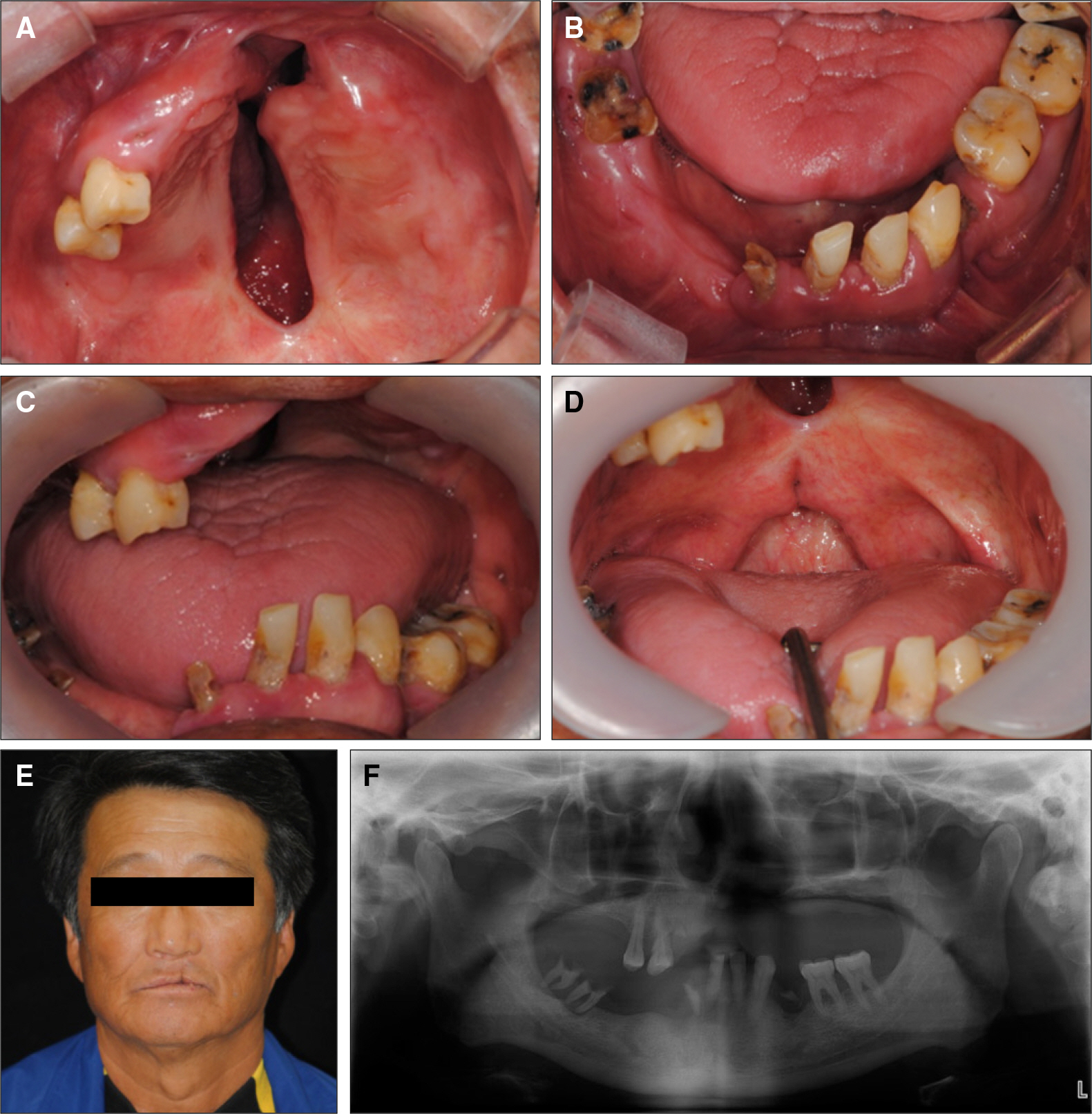
Fig. 1. Initial photographs. A: Maxillary occlusal view. There is linear defect on anterior alveolus and hard palate, B: Mandibular occlusal view, C: Frontal view. D: There is defect on soft palate and pharyngeal portion, E: Extraoral view, F: Panoramic radiograph.
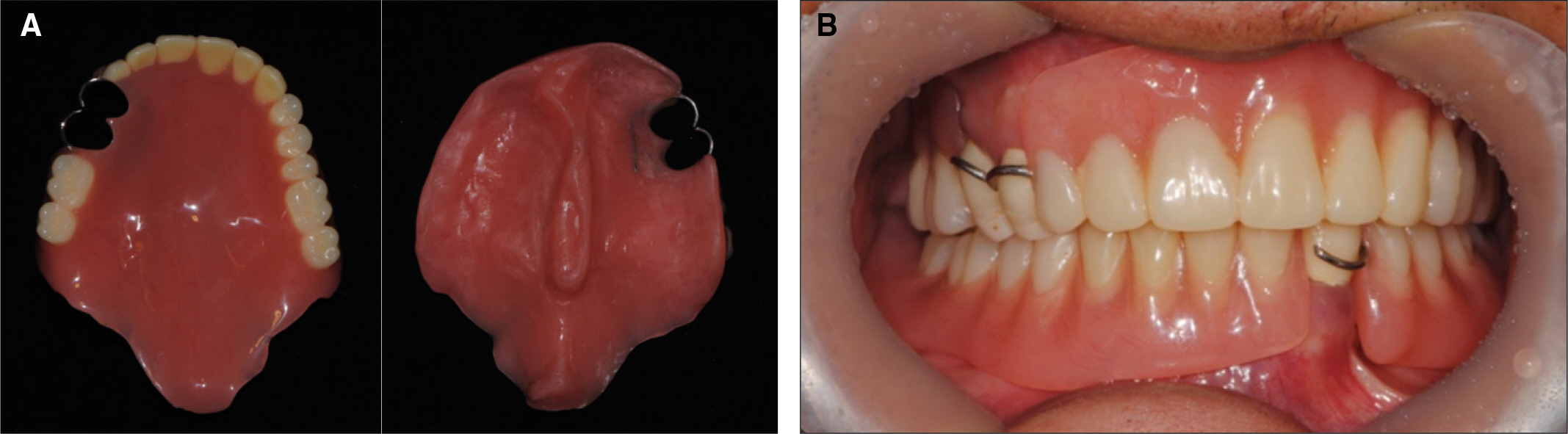
Fig. 2. A: Temporary denture, B: Intraoral photograph after the placement of temporary denture and crown.

Fig. 3. Final impression. A: Upper functional impression including velar and pharyngeal portion, B: Lower functional impression.

Fig. 4. Master cast. A: Upper master cast including velar and pharyngeal portion, B: Lower master cast.

Fig. 5. Metal framework. A: Upper framework including velar and pharyngeal part, B: Lower framework.

Fig. 6. Jaw relation registration procedure. A: Centric relation taking, B: Facebow transfer.

Fig. 7. Wax denture try in. A: Frontal view, B: Maxillary occlusial view. C: Functional impression of vealr and pharyngeal portions, taken by tissue conditioner (arrow point).
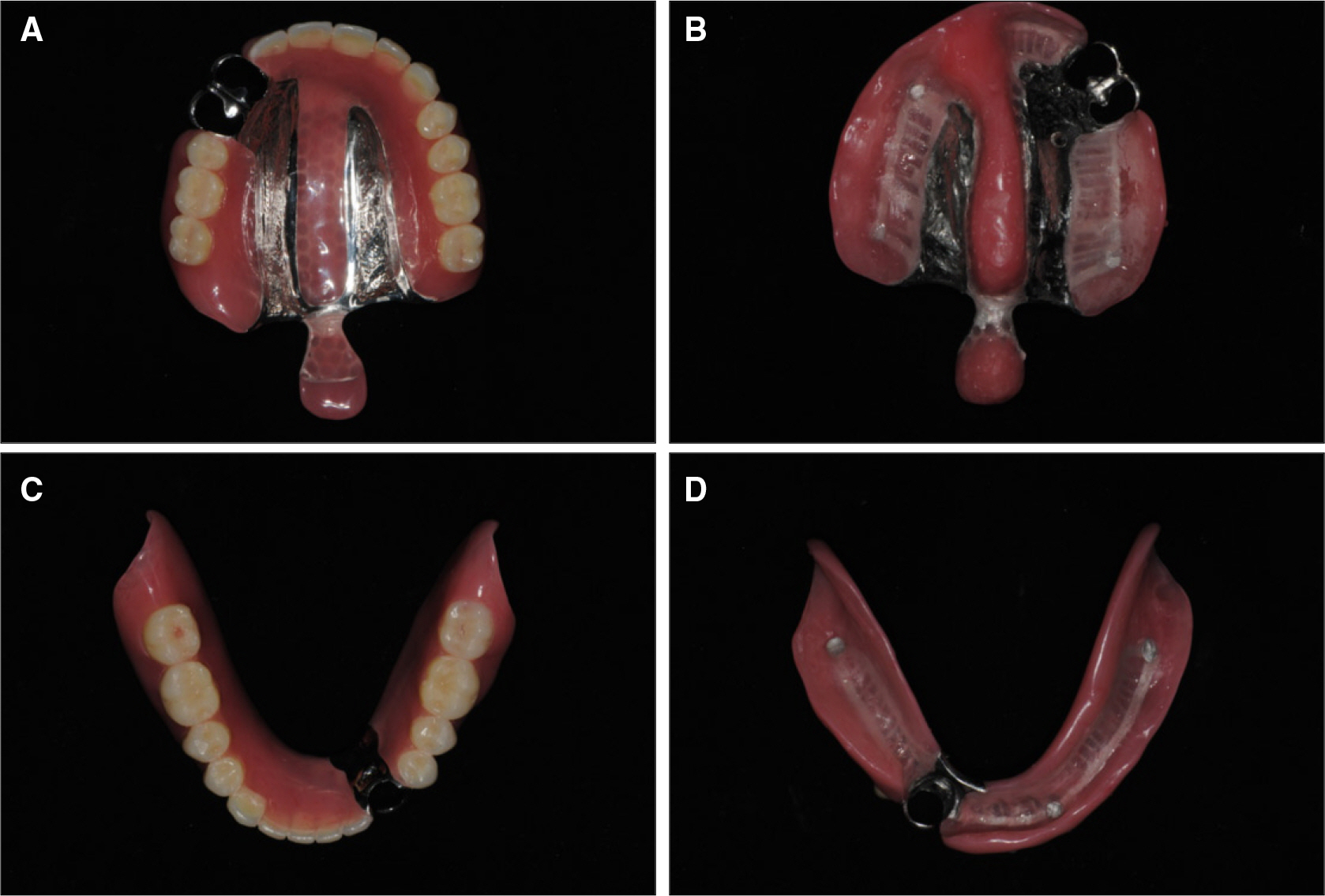
Fig. 8. Definitive prostheses. A, B: Upper definitive obturator, C, D: Lower definitive denture.
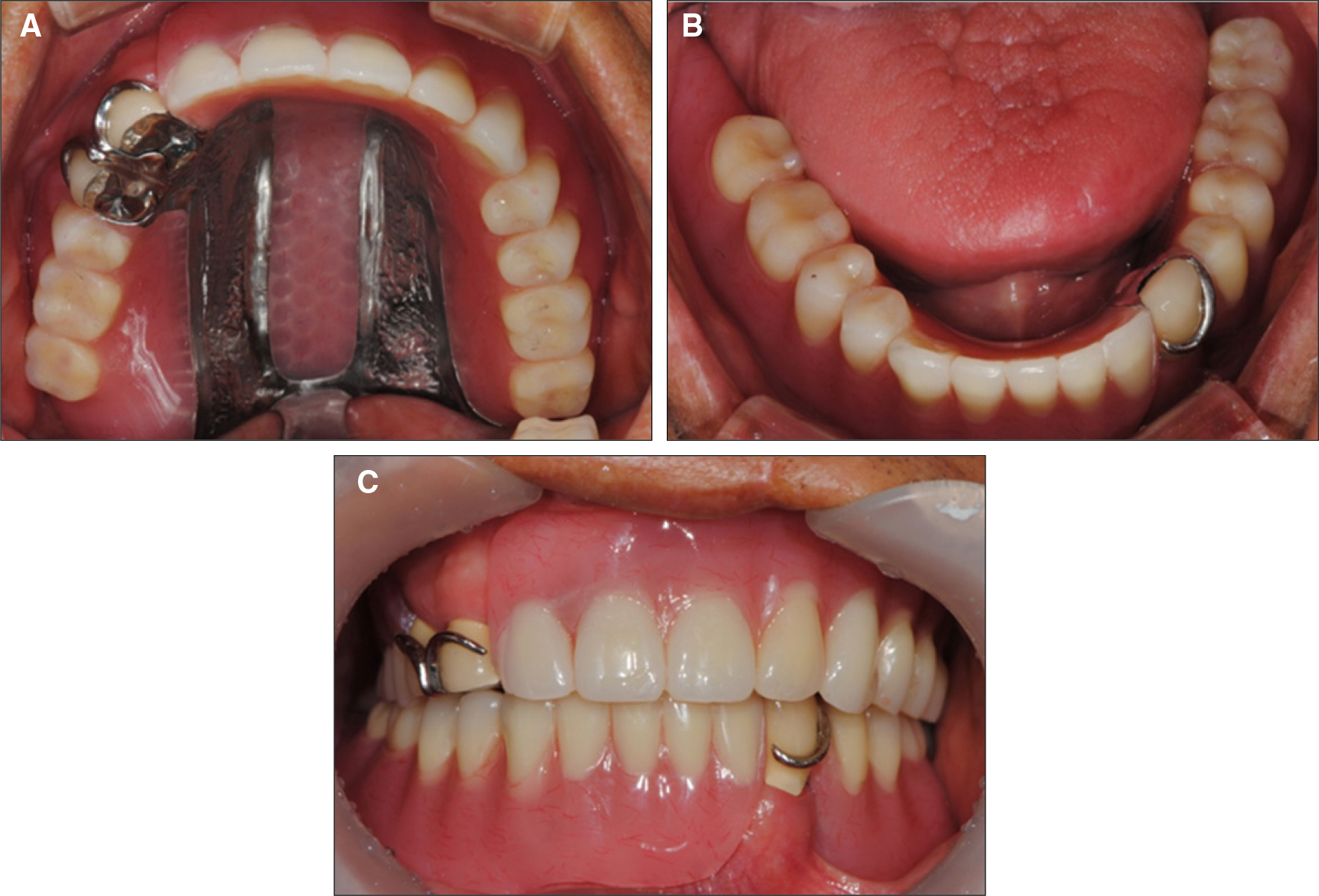
Fig. 9. Intraoral photograohs after the placement of definitive prosthese. A: Maxillary occlusal view, B: Mandibualar occlusal view, C: Frontal view.
Reference
-
1.Vojvodic D., Jerolimov V., Celebic A. Prosthetic rehabilitation of a cleft palate patient: a clinical report. J Prosthet Dent. 1996. 76:230–2.
Article2.Veau V., Borel S. Division palatine; anatomie, chirugie, phone-tique. Paris, Masson et cie;1931.3.Baik HS., Keem JH., Kim DJ. The prevalence of cleft lip and/or cleft palate in Korean male adult. Korean J Orthod. 2001. 31:63–9.4.Olinger NA. Cleft palate prosthesis rehabilitation. J Prosthet Dent. 1952. 2:117–35.
Article5.Brown KE. Peripheral consideration in improving obturator retention. J Prosthet Dent. 1968. 20:176–81.
Article6.Khan Z. Soft palate obturator prosthesis made with visible light-cured resin. J Prosthet Dent. 1989. 62:671–3.
Article7.Desjardins RP. Obturator prosthesis design for acquired maxillary defects. J Prosthet Dent. 1978. 39:424–35.
Article8.Casey DM. Palatopharyngeal anatomy and physiology. J Prosthet Dent. 1983. 49:371–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prosthetic treatment of velopharyngeal insufficiency using maxillary obturator in an edentulous patient with Passavant’s ridge
- Management of Swallowing and Speech Problems in Patients with Cleft Lip and Palate
- Interim palatal lift prosthesis as a constituent of multidisciplinary approach in the treatment of velopharyngeal incompetence
- Usefulness of Speech Therapy for Patients with Submucous Cleft Palate Treated with Furlow Palatoplasty
- Postoperative Speech Improvement in the Patients of Velopharyngeal Dysfunction without Definite Cleft Palate
