Superior Labral Dimension of the Glenohumeral Joint on Direct MR Arthrography (MRA): Relationship with Presence of SLAP (Superior Labrum Anterior to Posterior) Lesion
- Affiliations
-
- 1Department of Radiology, Seoul National University Bundang Hospital, Gyeonggi-do, Korea. jachoi88@gmail.com
- 2Department of Radiology, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Radiology, Hallym University Dongtan Sacred Heart Hospital, Gyeonggi-do, Korea.
- 4Department of Orthopaedic Surgery, Seoul National University Bundang Hospital, Gyeonggi-do, Korea.
- KMID: 1999918
- DOI: http://doi.org/10.13104/jksmrm.2014.18.3.193
Abstract
- PURPOSE
To evaluate the relationship between superior labral dimension of the glenohumeral joint on direct MRA and presence of SLAP lesion.
MATERIALS AND METHODS
IRB approval was obtained and informed consent was waived for this retrospective study. Direct MRA studies of the shoulder in 296 patients (300 shoulders) with arthroscopic surgery were analyzed by two radiologists blinded to the arthroscopic results, which were used as gold standard. One of the radiologists reviewed the images twice (session 1 and 2) for the evaluation of intra-observer variability. Transverse and longitudinal dimensions of superior labrum on coronal T1-weighted images were measured as base and height of the inverted triangular-shaped superior labrum and compared between patients with SLAP lesions vs. non-SLAP patients. Presence of meniscoid labrum was noted. Statistical analysis was done using unpaired t-test.
RESULTS
Among 279 patients (283 shoulders), 122 patients (43.1%) had SLAP lesions. The mean base/height of superior labrum in SLAP and non-SLAP patients measured on T1-weighted MR image were 8.8 mm / 5.2 mm, 8.5 mm / 4.9 mm for reader 1; 8.2 mm / 4.9 mm, 8.1 mm / 4.5 mm for session 1 of reader 2; 8.0 mm / 4.8 mm, 7.6 mm / 4.3 mm for session 2 of reader 2. In SLAP group, the mean labral height was larger than non-SLAP group with statistically significant difference (p<0.05). Fifteen patients (5.3%) had meniscoid labrum according to operation records.
CONCLUSION
In patients with SLAP lesion, the height of the superior glenoid labrum on oblique coronal image of MRA was slightly larger than non-SLAP patients. A larger height of superior glenoid labrum may be associated with SLAP lesions.
Keyword
MeSH Terms
Figure
-

Fig. 1 Measurement of superior labral dimension. (a) Superior labral dimension is measured on the plane where long head of biceps looks smallest and labrum largest twelve o'clock position. Transverse and longitudinal dimensions are obtained by measuring base (solid line) and height (dotted line) of inverted triangular shaped labrum. (b) On T1-weighted oblique coronal MRI, the base and height of the superior labrum are measured.

Fig. 2 65-year-old female with rotator cuff tear. (a) Triangular shaped superior labrum attached to glenoid rim is seen on oblique coronal T1-weighted MR image. The height of the labrum is measured to be 6.4 mm. (b) There is neither meniscoid labrum nor SLAP on arthroscopy.
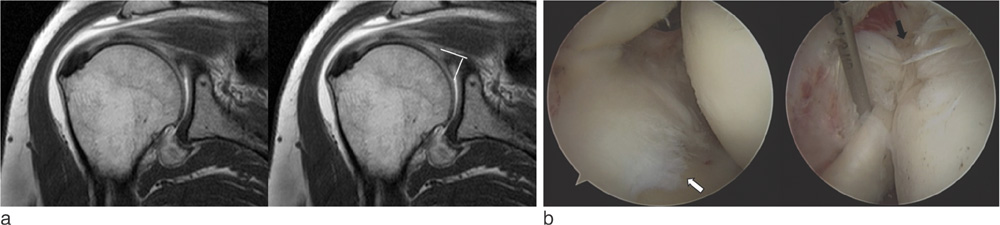
Fig. 3 55-year-old female with rotator cuff tear and SLAP. (a) The height of labrum is measured to be 10.3 mm on oblique coronal T1-weighted MR image. It is considered to be larger than usual. (b) On arthroscopy, both meniscoid labrum (white arrow) and SLAP (black arrow) are detected. The superior labrum is covering upper quarter of the glenoid.
Reference
-
1. Bencardino JT, Beltran J, Rosenberg ZS, et al. Superior labrum anterior-posterior lesions: diagnosis with MR arthrography of the shoulder. Radiology. 2000; 214:267–271.2. Vangsness CT Jr, Jorgenson SS, Watson T, Johnson DL. The origin of the long head of the biceps from the scapula and glenoid labrum. An anatomical study of 100 shoulders. J Bone Joint Surg Br. 1994; 76:951–954.3. Lee SB, Harryman DT 2nd. Superior detachment of a glenoid labrum variant resembling an incomplete discoid meniscus in a wheelchair ambulator. Arthroscopy. 1997; 13:511–514.4. Snyder SJ, Banas MP, Karzel RP. An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg. 1995; 4:243–248.5. Kanatli U, Ozturk BY, Bolukbasi S. Anatomical variations of the anterosuperior labrum: prevalence and association with type II superior labrum anterior-posterior (SLAP) lesions. J Shoulder Elbow Surg. 2010; 19:1199–1203.6. Kreitner KF, Botchen K, Rude J, Bittinger F, Krummenauer F, Thelen M. Superior labrum and labral-bicipital complex: MR imaging with pathologic-anatomic and histologic correlation. AJR Am J Roentgenol. 1998; 170:599–605.7. De Maeseneer M, Van Roy F, Lenchik L, et al. CT and MR arthrography of the normal and pathologic anterosuperior labrum and labral-bicipital complex. Radiographics. 2000; 20:S67–S81.8. Tischer T, Vogt S, Kreuz PC, Imhoff AB. Arthroscopic anatomy, variants, and pathologic findings in shoulder instability. Arthroscopy. 2011; 27:1434–1443.9. Connell DA, Potter HG, Wickiewicz TL, Altchek DW, Warren RF. Noncontrast magnetic resonance imaging of superior labral lesions 102 cases confirmed at arthroscopic surgery. Am J Sports Med. 1999; 27:208–213.10. Cooper DE, Arnoczky SP, O'Brien SJ, Warren RF, DiCarlo E, Allen AA. Anatomy, histology, and vascularity of the glenoid labrum. An anatomical study. J Bone Joint Surg Am. 1992; 74:46–52.11. Ilahi OA, Labbe MR, Cosculluela P. Variants of the anterosuperior glenoid labrum and associated pathology. Arthroscopy. 2002; 18:882–886.12. Ide J, Maeda S, Takagi K. Normal variations of the glenohumeral ligament complex: an anatomic study for arthroscopic Bankart repair. Arthroscopy. 2004; 20:164–168.13. Waldt S, Metz S, Burkart A, et al. Variants of the superior labrum and labro-bicipital complex: a comparative study of shoulder specimens using MR arthrography, multi-slice CT arthrography and anatomical dissection. Eur Radiol. 2006; 16:451–458.14. Smith AM, McCauley TR, Jokl P. SLAP lesions of the glenoid labrum diagnosed with MR imaging. Skeletal Radiol. 1993; 22:507–510.15. Davidson PA, Rivenburgh DW. Mobile superior glenoid labrum: a normal variant or pathologic condition? Am J Sports Med. 2004; 32:962–966.16. Zanetti M, Carstensen T, Weishaupt D, Jost B, Hodler J. MR arthrographic variability of the arthroscopically normal glenoid labrum: qualitative and quantitative assessment. Eur Radiol. 2001; 11:559–566.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Superior Labrum Anterior to Posterior (SLAP) Lesion with Glenohumeral Instability
- Superior Labrum Anterior to Posterior Lesion Type II with Accompanied Findings: Assessment of Shoulder MR Arthrographic Findings
- Is There a Clinically Important Superior Labrum Anterior to Posterior (SLAP) Lesion?
- MIR Arthrography of the Labral-Capular-Ligamentous Complex : Normal Variations and Pitfalls
- Rare Normal Variation Between Biceps Anchor and Superior Labrum: A Case Report
