Korean J Urol.
2006 Apr;47(4):381-386. 10.4111/kju.2006.47.4.381.
The Correlation between the Prostatic Morphology Seen on Cystourethroscopy, the Clinical Findings and the Outcomes of Transurethral Resection of the Prostate
- Affiliations
-
- 1Department of Urology, Wonkwang University School of Medicine, Iksan, Korea.
- KMID: 1997147
- DOI: http://doi.org/10.4111/kju.2006.47.4.381
Abstract
- PURPOSE
Cystourethroscopy provides information on the cause, size and severity of obstruction and the patency of the bladder neck, prostatic occlusion of the urethra and the estimated prostatic size. We evaluated the relationship between the prostatic morphology on the cystourethroscopic findings and the clinical findings and the outcomes of transurethral resection of the prostate (TURP).
MATERIALS AND METHODS
We evaluated 291 patients who underwent TURP between January 1999 and June 2004. The prostate volume, the preoperative maximal flow rate (MFR), the postvoid residual urine volume (PVR) and the International Prostate Symptom Score (IPSS) were determined. The patients were divided into 4 groups by the cystourethroscopic findings before TURP: group I - isolated middle lobe enlargement, group II - isolated lateral lobe enlargement, group III - middle and lateral lobe enlargement, group IV - posterior commissural hyperplasia (median bar type).
RESULTS
The analyses included 250 patients who had a mean age of 71.2 years, a mean prostate volume of 46.2g, a mean preoperative MFR of 7.8ml/s, a PVR of 73.1ml and an IPSS of 25.6. The prostate volume was larger in group II and III than in group l. The preoperative MFR and IPSS were not correlated with the prostatic morphology, but the storage symptom score was significantly higher in group IV. The postoperative parameters were not correlated with the prostatic morphology noted on cystourethroscopy.
CONCLUSIONS
The cystourethroscopic findings are not prognostic factors for the expected surgical outcomes in TURP. TURP is a good surgical therapeutic tool for treating benign prostatic hyperplasia regardless of the prostatic morphology seen on cystourethroscopy. Cystourethroscopy might need to be performed only in limited cases.
Keyword
MeSH Terms
Figure
-
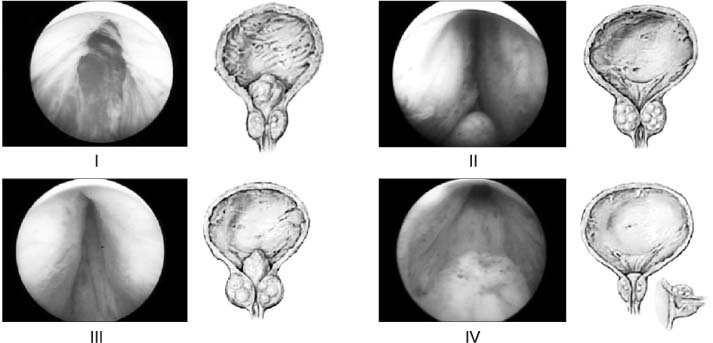
Fig. 1 Gross appearance of hyperplastic prostatic gland. I: isolated middle lobe enlargement, II: isolated lateral lobe enlargement, III: middle and lateral lobe enlargement, IV: posterior commissural hyperplasia.
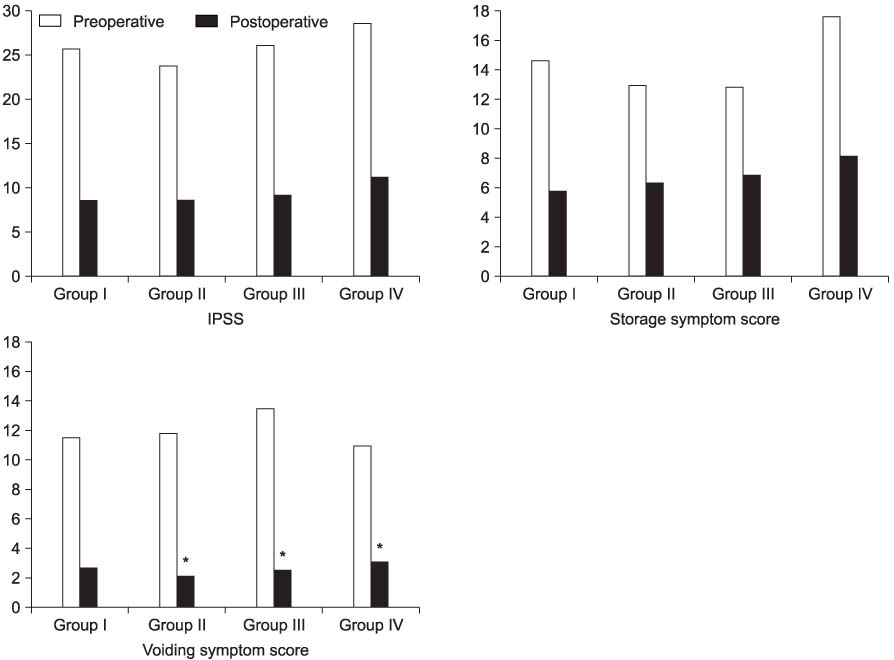
Fig. 2 Comparison of the preoperative and postoperative symptom scores between groups. IPSS: International Prostate Symptom Score, *: p<0.05 by Duncan's multiple comparison test.
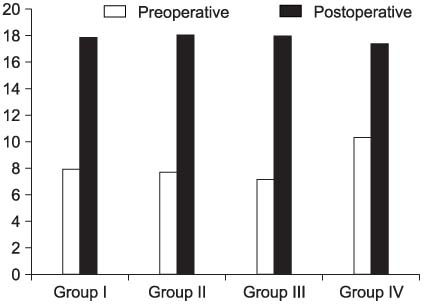
Fig. 3 Comparison of the preoperative and postoperative maximal flow rates (ml).
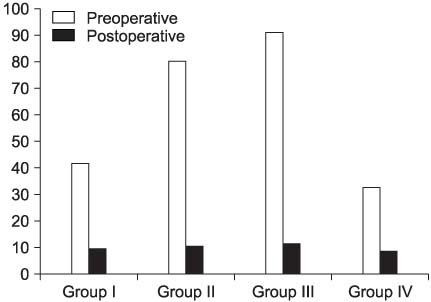
Fig. 4 Comparison of the preoperative and postoperative postvoid residual urine volumes (ml).
Reference
-
1. AUA Practice Guidelines Committee. AUA guideline on management of benign prostatic hyperplasia (2003). Chapter 1: Diagnosis and treatment recommendations. J Urol. 2003. 170:530–547.2. Plorde JJ, Kennedy RP, Bourne HH, Ansell JS, Petersdorf RG. Course and prognosis of prostatectomy: with a note on the incidence of bacteremia and effectiveness of chemoprophylaxis. N Engl J Med. 1965. 272:269–277.3. Neal DE, Ramsden PD, Sharples L, Smith A, Powell PH, Styles RA, et al. Outcome of elective prostatectomy. BMJ. 1989. 299:762–767.4. Ignjatovic I. Prediction of unfavourable symptomatic outcome of transurethral prostatectomy in patients with the relative indication for operation. Int Urol Nephrol. 1997. 29:653–660.5. Kuo HC, Chang SC, Hsu T. Predictive factors for successful surgical outcome of benign prostatic hypertrophy. Eur Urol. 1993. 24:12–19.6. Kim GW, Kim CI, Lee SC. Predictive factors for successful surgical outcome of benign prostatic hypertrophy. Korean J Urol. 1995. 36:417–424.7. Roehrborn CG, McConnell JD. Walsh PC, Retik AB, Vaughan ED, Wein AJ, editors. Etiology, pathophysiology, epidemiology, and natural history of benign prostatic hyperplasia. Campbell's urology. 2002. 8th ed. Philadelphia: Saunders;1297–1336.8. Madsen FA, Bruskewitz RC. Cystoscopy in the evaluation of benign prostatic hyperplasia. World J Urol. 1995. 13:14–16.9. Chatelain C, Denis L, Foo KT, Khoury S, McConnell JD, Abrams P, et al. Chatelain C, Denis L, Foo KT, McConnell JD, editors. Evaulation and treatment of lower urinary tract symptoms (LUTS) in older men. Fifth international consultation on benign prostatic hyperplasia. 2001. UK: Health Publication Ltd;519–534.10. McConnell JD, Barry MJ, Bruskewitz RC, Bueschen AJ, Denston SE, Holtgrewe HL, et al. McConnell JD, editor. Benign prostatic hyperplasia: diagnosis and treatment. Clinical Practice Guideline No 8 (AHCRP Publication No 94-0582). Rockville. 1994. Maryland: US Dept. of Health and Human Services;1–17.11. el Din KE, de Wildt MJ, Rosier PF, Wijkstra H, Debruyne FM, de la Rosette JJ. The correlation between urodynamic and cystoscopic findings in elderly men with voiding complaints. J Urol. 1996. 155:1018–1022.12. Kim HJ, Seo BW, Park YH. The relationship of prostatic urethral obstruction of cystourethroscopy with voiding symptoms and prostate volume in lower urinary tract symptoms patients. Korean J Urol. 2000. 41:47–51.13. Simonsen O, Moller-Madsen B, Dorflinger T, Norgaard JP, Jorgensen HS, Lundhus E. The significance of age on symptoms and urodynamic- and cystoscopic findings in benign prostatic hypertrophy. Urol Res. 1987. 15:355–358.14. Bosch JL, Kranse R, van Mastrigt R, Schroder FH. Reasons for the weak correlation between prostate volume and urethral resistant parameters in patients with prostatism. J Urol. 1995. 153:689–693.15. Kojima M, Naya Y, Inoue W, Ukimura O, Watanabe M, Saitoh M, et al. The American Urological Association symptom index for benign prostatic hyperplasia as a function of age, volume and ultrasonic appearance prostate. J Urol. 1997. 157:2160–2165.16. Roehrborn CG, McConnell JD, Saltzman B, Bergner D, Gray T, Narayan P, et al. Storage (irritative) and voiding (obstructive) symptoms as predictors of benign prostatic hyperplasia progression and related outcomes. Eur Urol. 2002. 42:1–6.17. Grayhack JT, Kozlowski JM, Lee C. The pathogenesis of benign prostatic hyperplasia: a proposed hypothesis and critical evaluation. J Urol. 1998. 160:2375–2380.18. Rho SH, Lee DH, Sim BS. The efficacy of transurethral resection of prostate in the patients with benign prostatic hyperplasia of 30gm or less. Korean J Urol. 2002. 43:1051–1054.19. Barry MJ, Cockett AT, Holtgrewe HL, McConnell JD, Sihelnik SA, Winfield HN. Relationship of symptoms of prostatism to commonly used physiological and anatomical measures of the severity of benign prostatic hyperplasia. J Urol. 1993. 150:351–358.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Observation on Transurethral Resection of Prostate and Suprapubic Prostatectomy for Benign Prostatic Hypertrophy
- Fluid extravasation caused by bladder perforation during bipolar transurethral resection using saline solution: a case report
- Comparison of the Finding of Transrectal Ultrasonography and the Result of Transurethral Resection of Prostate according to the Histologic Types in Benign Prostatic Hyperplasia
- Clinical Observation of Prostatic Abscess found during Tranaurethral Resection of Prostate
- Clinical Results of Transurethral Resection for the Benign Prostatic Hypertrophy -Significance of Suprapubic Cystostomy before Transurethral Resection-
