Kosin Med J.
2012 Jun;27(1):31-36. 10.7180/kmj.2012.27.1.31.
Clinical Outcome of Positive Margin of Postgastrectomy with Adenocarcinoma of Stomach
- Affiliations
-
- 1Department of Surgery, College of Medicine, Kosin University, Busan, Korea. gslsh@ns.kosinmed.or.kr
- KMID: 1993584
- DOI: http://doi.org/10.7180/kmj.2012.27.1.31
Abstract
OBJECTIVES
Many investigators have recommended adequate resection margin and lymphadenectomy for radical curative resection. The aim of this study is to evaluate clinical characteristics of positive resection margin (proximal or distal) of postgastrectomy in advanced gastric cancer.
METHODS
We studied 17 patients with gastric cancer who were diagnosed positive resection margin by intraoperative frozen biopsy or permanent biopsy report from January 2005 to December 2007, retrospectively. Surgical margin monitored by endoscopy.
RESULTS
Distal gastrectomy was performed in 13 patients and total gastrectomy in 4. Gastrectomy with combined resection including splenectomy was performed in 3, distal pancreatectomy in 2, transverse colon segmental resection in 1, and cholecystectomy in 2. Positive Proximal margin was found in 12, positive distal margin in 3, and both in 2. Palliative chemotherapy was performed in 8 patients. Postoperative follow up endoscopy was established in only 8 patients. Malignant results from endoscopic biopsy in gastroenteric or esophagoenteric anastomotic line were proven in 2 patients during follow up. 9 patients were not performed follow-up endoscopy. Among total 17 patients, 2 patients are alive. Fifteen patients died of aggravation of disease in 13 and postoperative complication in 2.
CONCLUSIONS
Although positive surgical margin in far advanced gastric cancer were found, it can consider that does not further resection to obtain microscopic clear anastomotic margin.
MeSH Terms
Figure
-

Fig. 1 Types of reconstruction after gastric surgery of the stage IV patient

Fig. 2 Positive surgical margin of the reconstruction type
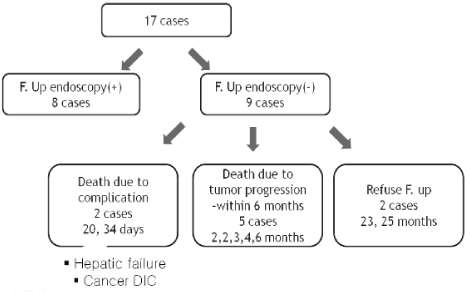
Fig. 3 Prognosis of margin positive case

Fig. 4 Prgnosis of margin positive case followed by endoscopy
Cited by 1 articles
-
Application of Raman spectroscopy in breast cancer surgery
Yikeun Kim, Sung Ui Jung, Jinhyuk Choi
Kosin Med J. 2023;38(3):176-183. doi: 10.7180/kmj.23.129.
Reference
-
1. Seo YJ, Bae JM, Kim SW, Song SK. Different clinical outcomes of stage IV gastric cancer according to the curability of surgery. J Korean Surg Soc. 2009. 77:170–176.
Article2. Helyer LK, O'Brien C, Coburn NG, Swallow CJ. Surgeons' knowledge of quality indicators for gastric cancer surgery. Gastric Cancer. 2007. 10:205–214.
Article3. Shen JG, Cheong JH, Hyung WJ, Kim J, Choi SH, Noh SH. Influence of a microscopic positive proximal margin in the treatment of gastric adenocarcinoma of the cardia. World J Gastroenterol. 2006. 12:3883–3886.
Article4. Cho BC, Jeung HC, Choi HJ, Rha SY, Hyung WJ, Cheong JH, et al. Prognostic impact of resection margin involvement after extended (D2/D3) gastrectomy for advanced gastric cancer: a 15-year experience at a single institute. J Surg Oncol. 2007. 95:461–468.
Article5. Bozzetti F. Principles of surgical radicality in the treatment of gastric cancer. Surg Oncol Clin N Am. 2001. 10:833–854.
Article6. Sillah K, Griffiths EA, Pritchard SA, Swindell R, West CM, Page R, et al. Clinical impact of tumour involvement of the anastomotic doughnut in oesophagogastric cancer surgery. Ann R Coll Surg Engl. 2009. 91:195–200.
Article7. Hahn KH, Yang HK, Kim JP. Clinical Evaluation of Routine Frozen Section Study of Resection Margin in Curative Gastric Surgery. J Korean Surg Soc. 1997. 52:328–334.8. Cho YK, Chang JK, Hong KC, Park HG, Lee CY, Sohn JH, et al. Clinicopathlogic study on cases with positive resection margin in gastrectomy for stomach cancer. J Korean Surg Soc. 1990. 38:572–576.9. Jeong GA, Cho GS, Lee MS, Kim YJ, Kang KH, Kim HS, et al. Usefulness of reoperation after recurrence of gastric cancer. J Korean Surg Soc. 2009. 77:96–105.
Article10. Wang SY, Yeh CN, Lee HL, Liu YY, Chao TC, Hwang TL, et al. Clinical impact of positive surgical margin status on gastric cancer patients undergoing gastrectomy. Ann Surg Oncol. 2009. 16:2738–2743.
Article11. Sun Z, Li DM, Wang ZN, Huang BJ, Xu Y, Li K, et al. Prognostic significance of microscopic positive margins for gastric cancer patients with potentially curative resection. Ann Surg Oncol. 2009. 16:3028–3037.
Article12. Ikeguchi M, Katano K, Oka A, Tsujitani S, Maeta M, Kaibara N. The proliferative activity of cancer cells at the invasive margin of a tumor is a good indicator of the prognosis of patients with gastric cancer with serosal invasion. Int Surg. 1996. 81:122–125.13. Bozzetti F, Bonfanti G, Regalia E, Andreola S, Doci R, La Malfa G, et al. How long is a 6 cm margin of resection in the stomach? Eur J Surg Oncol. 1992. 18:481–483.14. Papachristou DN, Agnanti N, D'Agostino H, Fortner JG. Histologically positive esophageal margin in the surgical treatment of gastric cancer. Am J Surg. 1980. 139:711–713.
Article15. Gall CA, Rieger NA, Wattchow DA. Positive proximal resection margins after resection for carcinoma of the oesophagus and stomach: effect on survival and symptom recurrence. Aust N Z J Surg. 1996. 66:734–737.
Article16. Chan WH, Wong WK, Khin LW, Chan HS, Soo KC. Significance of a positive oesophageal margin in stomach cancer. Aust N Z J Surg. 2000. 70:700–703.
Article17. Tsujitani S, Okuyama T, Orita H, Kakeji Y, Maehara Y, Sugimachi K, et al. Margins of resection of the esophagus for gastric cancer with esophageal invasion. Hepatogastroenterology. 1995. 42:873–877.18. Fujimoto S, Takahashi M, Mutou T, Kobayashi K, Toyosawa T, Ohkubo H. Clinicopathologic characteristics of gastric cancer patients with cancer infiltration at surgical margin at gastrectomy. Anticancer Res. 1997. 17:689–694.19. Song KY, Hyung WJ, Kim HH, Han SU, Cho GS, Ryu SW, et al. Korean Laparoscopic Gastrointestinal Surgery Study (KLASS) Group. Is gastrectomy mandatory for all residual or recurrent gastric cancer following endoscopic resection? A large-scale Korean multi-center study. J Surg Oncol. 2008. 98:6–10.
Article20. Volpe CM, Driscoll DL, Douglass HO Jr. Outcome of patients with proximal gastric cancer depends on extent of resection and number of resected lymph nodes. Ann Surg Oncol. 2000. 7:139–144.
Article21. de Gara CJ, Hanson J, Hamilton S. A population-based study of tumor-node relationship, resection margins, and surgeon volume on gastric cancer survival. Am J Surg. 2003. 186:23–27.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Immunohistochemical Studies on Localization of Carcinoembryonic Antigen and Epithelial Membrane Antigen in Adenoma and Well-differentiated Adenocarcinoma of the Stomach
- Postgastrectomy Bezoar Due to Suture Thread
- Collision of Adenocarcinoma and Schwannoma of the Stomach: A Case Report
- Interpretation of Pathologic Margin after Endoscopic Resection of Gastrointestinal Stromal Tumor
- Papillary gastric adenocarcinoma
