Korean J Obstet Gynecol.
2012 Jul;55(7):493-501. 10.5468/KJOG.2012.55.7.493.
Laparoscopic cervical myomectomy: Five years of experience
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Cheil General Hospital and Women's Healthcare Center, Kwandong University College of Medicine, Seoul, Korea. dr66205@naver.com
- 2Department of Obstetrics and Gynecology, Dong-A University Medical Center, Dong-A University College of Medicine, Busan, Korea.
- KMID: 1992559
- DOI: http://doi.org/10.5468/KJOG.2012.55.7.493
Abstract
OBJECTIVE
This retrospective case series evaluated the feasibility and safety of laparoscopic cervical myomectomy.
METHODS
Sixty-five patients with cervical myoma who underwent laparoscopic cervical myomectomy were included in this study.
RESULTS
The mean age of the patients was 39.2 +/- 6.0 years. The marriage rate was 67.7%, and the mean parity was 1.09. The most common symptoms in the patients were increased myoma size (41.5%) and menorrhagia (13.8%), while 20% of patients were asymptomatic. The average diameter of the myomas treated was 72.68 +/- 20.28 mm, and the mean number of myomas per patient was 1.41 +/- 0.88. Laparoscopic cervical myomectomy required a mean time of 63.25 +/- 20.34 minutes. The difference between preoperative and postoperative hemoglobin levels was 2.01 +/- 0.73 g/dL, and no patient required transfusion or conversion to laparotomy.
CONCLUSION
Sixty-five procedures of laparoscopic cervical myomectomy were performed safely. Operation time and complications were minimal. With correct understanding of pelvic anatomy, laparoscopic cervical myomectomy can be carried out safely and easily, and represents a minimally invasive treatment choice for symptomatic cervical myoma.
MeSH Terms
Figure
-

Fig. 1 Laparoscopic cervical myomectomy: posterior cervical myoma, subserosal type. Before enucleation of myoma, ureter dissection was perfomed. After enucleation, incised peritoneum was sutured continuously.
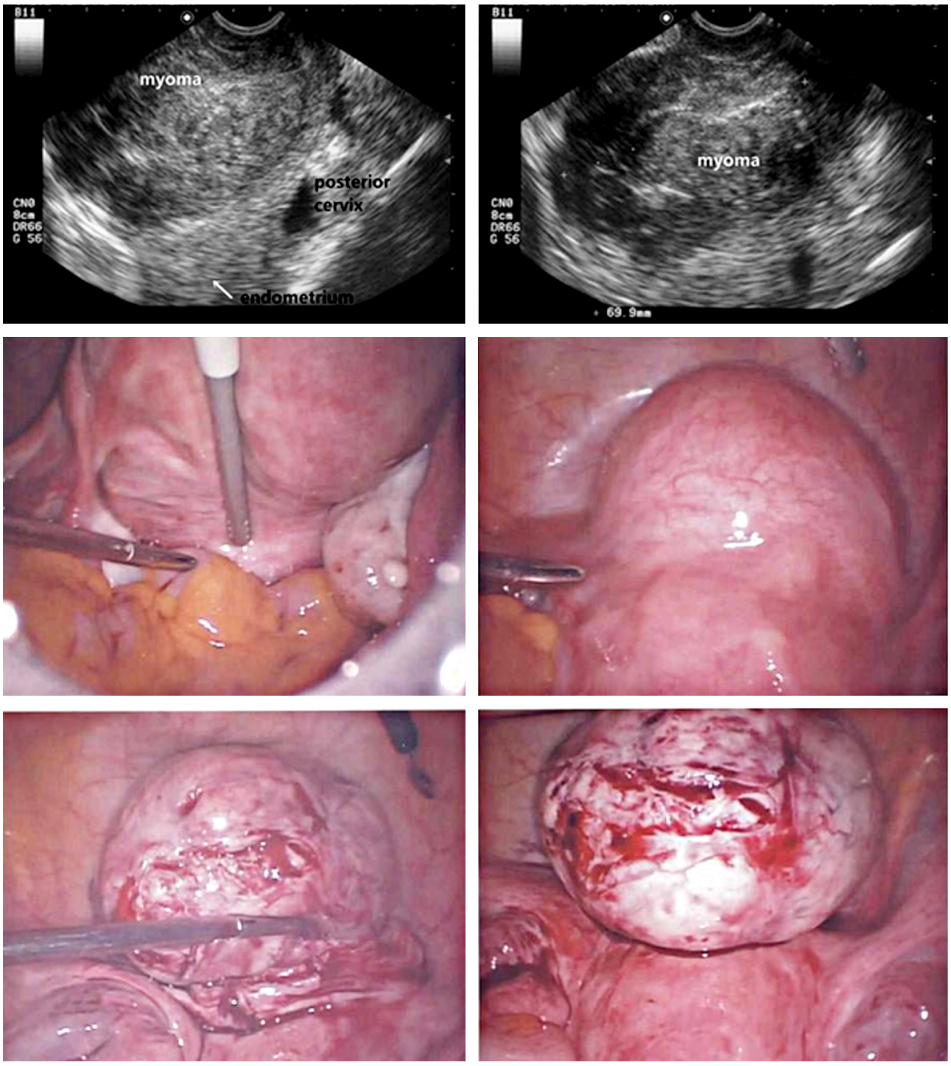
Fig. 2 Laparoscopic cervical myomectomy: anterior cervical myoma, intracervical type. Adequate separation of the bladder was performed before myoma enucleation. In this case, the anterior cervix was incised to remove the myoma. After enucleation of the myoma, the incised cervix was sutured continuously in 2 layers.
Reference
-
1. Adams Hillard PJ. Berek JS, Novak E, editors. Benign diseases of the female reproductive tract. Berek & Novak's gynecology. 2007. 14th ed. Philadelphia (PA): Lippincott Williams & Wilkins;469–481.2. Istre O. Management of symptomatic fibroids: conservative surgical treatment modalities other than abdominal or laparoscopic myomectomy. Best Pract Res Clin Obstet Gynaecol. 2008. 22:735–747.3. Hurst BS, Matthews ML, Marshburn PB. Laparoscopic myomectomy for symptomatic uterine myomas. Fertil Steril. 2005. 83:1–23.4. Stovall TG. Mann WJ, Stovall TG, editors. Myomectomy. Gynecologic surgery. 1996. New York (NY): Churchill Livingstones;445–461.5. Takeuchi H, Kitade M, Kikuchi I, Shimanuki H, Kumakiri J, Kobayashi Y, et al. A new enucleation method for cervical myoma via laparoscopy. J Minim Invasive Gynecol. 2006. 13:334–336.6. Semm K, Mettler L. Technical progress in pelvic surgery via operative laparoscopy. Am J Obstet Gynecol. 1980. 138:121–127.7. American College of Obstetricians and Gynecologists (ACOG). Clinical Management Guidelines for the Obstetrician-Gynecologist. Surgical alternatives to hysterectomy in the management of leiomyomas. 2004 Compendium of Selected Publications. 2004. Washington, DC: ACOG;665–673. Number 16, May 2000.8. Seracchioli R, Rossi S, Govoni F, Rossi E, Venturoli S, Bulletti C, et al. Fertility and obstetric outcome after laparoscopic myomectomy of large myomata: a randomized comparison with abdominal myomectomy. Hum Reprod. 2000. 15:2663–2668.9. Seracchioli R, Manuzzi L, Vianello F, Gualerzi B, Savelli L, Paradisi R, et al. Obstetric and delivery outcome of pregnancies achieved after laparoscopic myomectomy. Fertil Steril. 2006. 86:159–165.10. Agdi M, Tulandi T. Endoscopic management of uterine fibroids. Best Pract Res Clin Obstet Gynaecol. 2008. 22:707–716.11. Dubuisso JB, Fauconnier A, Babaki-Fard K, Chapron C. Laparoscopic myomectomy: a current view. Hum Reprod Update. 2000. 6:588–594.12. Lee CL, Wang CJ. Laparoscopic myomectomy. Taiwan J Obstet Gynecol. 2009. 48:335–341.13. Glasser MH. Minilaparotomy myomectomy: a minimally invasive alternative for the large fibroid uterus. J Minim Invasive Gynecol. 2005. 12:275–283.14. Marret H, Chevillot M, Giraudeau B. Study Group of the French Society of Gynaecology and Obstetrics (Ouest Division). Factors influencing laparoconversions during the learning curve of laparoscopic myomectomy. Acta Obstet Gynecol Scand. 2006. 85:324–329.15. Jung US, Wie HJ, Yoon HJ, Kyung MS, Lee KW, Han JS, et al. Clinical efficacy of laparoscopic myomectomy for 110 cases of various sized myomas. Korean J Obstet Gynecol. 2007. 50:918–925.16. Dubuisson JB, Fauconnier A, Fourchotte V, Babaki-Fard K, Coste J, Chapron C. Laparoscopic myomectomy: predicting the risk of conversion to an open procedure. Hum Reprod. 2001. 16:1726–1731.17. Matsuoka S, Kikuchi I, Kitade M, Kumakiri J, Kuroda K, Tokita S, et al. Strategy for laparoscopic cervical myomectomy. J Minim Invasive Gynecol. 2010. 17:301–305.18. Chen I, Motan T, Kiddoo D. Gonadotropin-releasing hormone agonist in laparoscopic myomectomy: systematic review and meta-analysis of randomized controlled trials. J Minim Invasive Gynecol. 2011. 18:303–309.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hybrid laparoscopic myomectomy: A novel technique
- Clinical experience with single-port access laparoscopic cystectomy and myomectomy
- Disseminated Peritoneal Leiomyomatosis Following Previous Laparoscopic Myomectomy with Morcellation
- Surgical outcomes for robot-assisted laparoscopic myomectomy compared with laparoscopic myomectomy
- Repetitive Spontaneous Uterine Rupture in the First Trimester after Laparoscopic Myomectomy: A Case Report and Review of Literature
