Complete Atrioventricular Block due to Infective Endocarditis of Bicuspid Aortic Valve
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Uijeongbu St. Mary's Hospital, The Catholic University of Korea School of Medicine, Uijeongbu, Korea. jhkmht@gmail.com
- KMID: 1980368
- DOI: http://doi.org/10.4250/jcu.2011.19.3.140
Abstract
- A 38-year-old man visited our emergency department presenting with a 6-day persistent fever. The man had undergone an orthodontic procedure 7 days prior to the visit. He had a fever with a temperature of 38.2degrees C and a diastolic murmur (grade III) was detected at the left sternal border. Reddish-brown lines beneath the nails were present, and raised lesions which were red and painful were detected on the soles of the patient's feet. Laboratory findings showed an elevated inflammatory marker. Transthoracic and transesophageal echocardiograms, showed a bicuspid aortic valve, and moderate aortic regurgitation and vegetation were noted. Treatment with antibiotics was given, but 4 days later, a 12 lead electrocardiogram revealed complete atrioventricular (AV) block. Immediately, a temporary pacemaker was inserted, and the following day an aortic valve replacement was performed. Intraoperative findings revealed a fistula around the AV node. He has suffered no subsequent cardiac events during the follow-up.
Keyword
MeSH Terms
Figure
-
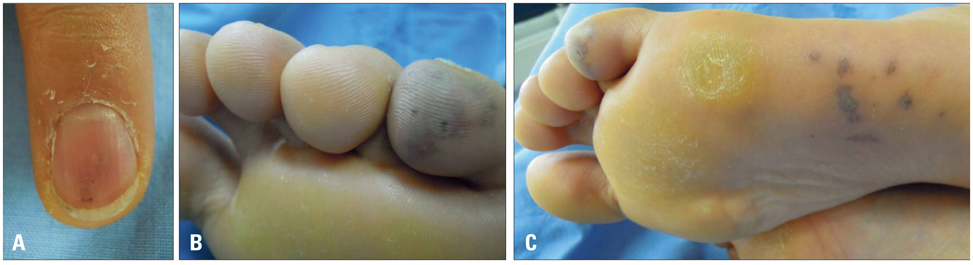
Fig. 1 A: Reddish-brown lines beneath the nails. B and C: Painful red raised lesion on the soles of the feet.
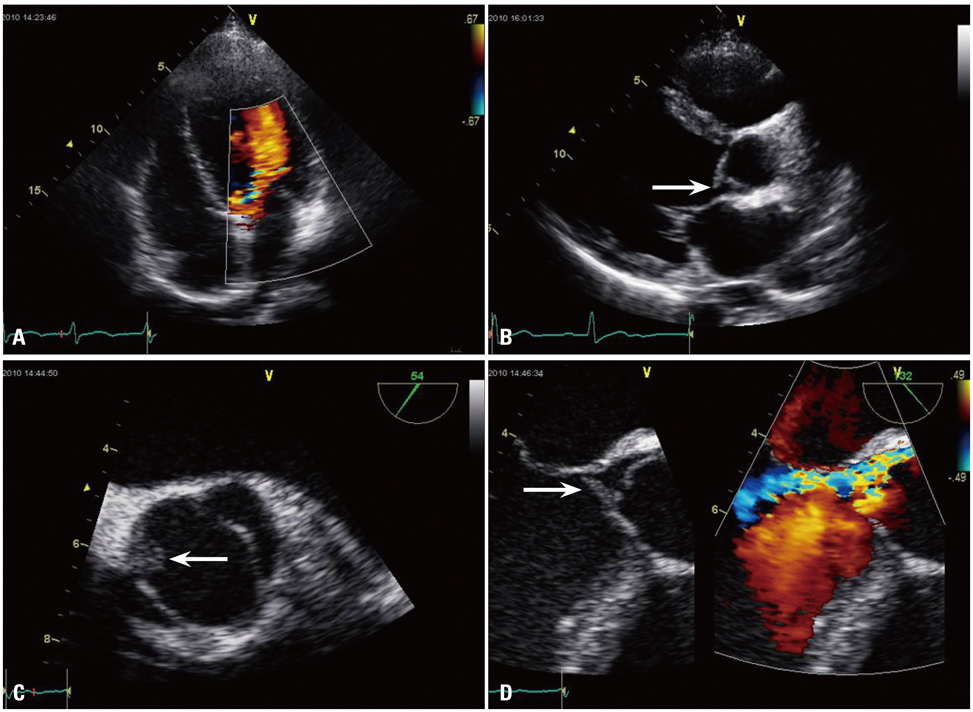
Fig. 2 Transthoracic and transesophageal echocardiography. A: Moderate aortic regurgitation on apical view. B: The presence of vegetation (arrow) in the aortic valve tip on parasternal long axis view. C: Two leaflets seen in the aortic valve on a transesophageal echocardiogram. The vegetation (arrow) is seen in the left leaflet. D: The presence of vegetation (arrow) in the aortic valve tip on a transesophageal echocardiogram. The presence of aortic regurgitation seen on Doppler echocardiogram.

Fig. 3 Electrocardiogram. A: Electrocardiogram on hospital day 4: complete atrioventricular block. B: Electrocardiogram on post-op day 30: normal sinus rhythm.

Fig. 4 Intraoperative and surgical pathology finding. A: Intraoperative finding: the presence of a fistula (arrow) around the atrioventricular node below the left cusp. B: Surgical pathology finding: two leaflets seen in the aortic valve. A 1.5 × 1.3 cm sized vegetation seen in a leaflet.
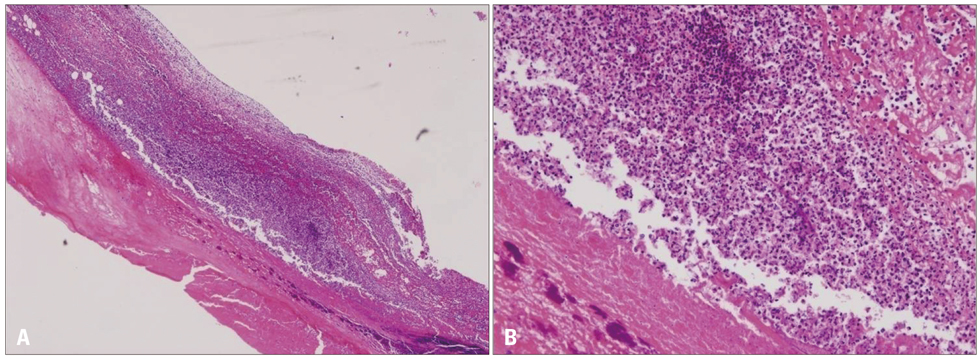
Fig. 5 Microscopic finding. Histologic exam shows aortic valve leaflet vegetation with many inflammation cell and necrotic tissue (A, H&E stain 50×) (B, H&E stain 200×).
Reference
-
1. Yener N, Oktar GL, Erer D, Yardimci MM, Yener A. Bicuspid aortic valve. Ann Thorac Cardiovasc Surg. 2002. 8:264–267.2. Knosalla C, Weng Y, Yankah AC, Siniawski H, Hofmeister J, Hammerschmidt R, Loebe M, Hetzer R. Surgical treatment of active infective aortic valve endocarditis with associated periannular abscess--11 year results. Eur Heart J. 2000. 21:490–497.
Article3. Ward C. Clinical significance of the bicuspid aortic valve. Heart. 2000. 83:81–85.
Article4. Kahveci G, Bayrak F, Pala S, Mutlu B. Impact of bicuspid aortic valve on complications and death in infective endocarditis of native aortic valves. Tex Heart Inst J. 2009. 36:111–116.5. Siu SC, Silversides CK. Bicuspid aortic valve disease. J Am Coll Cardiol. 2010. 55:2789–2800.
Article6. Lamas CC, Eykyn SJ. Bicuspid aortic valve--A silent danger: analysis of 50 cases of infective endocarditis. Clin Infect Dis. 2000. 30:336–341.
Article7. Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, Levison M, Bolger A, Cabell CH, Takahashi M, Baltimore RS, Newburger JW, Strom BL, Tani LY, Gerber M, Bonow RO, Pallasch T, Shulman ST, Rowley AH, Burns JC, Ferrieri P, Gardner T, Goff D, Durack DT. American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee. American Heart Association Council on Cardiovascular Disease in the Young. American Heart Association Council on Clinical Cardiology. American Heart Association Council on Cardiovascular Surgery and Anesthesia. Quality of Care and Outcomes Research Interdisciplinary Working Group. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007. 116:1736–1754.8. Graupner C, Vilacosta I, SanRomán J, Ronderos R, Sarriá C, Fernández C, Mújica R, Sanz O, Sanmartín JV, Pinto AG. Periannular extension of infective endocarditis. J Am Coll Cardiol. 2002. 39:1204–1211.
Article9. Arnett EN, Roberts WC. Valve ring abscess in active infective endocarditis. Frequency, location, and clues to clinical diagnosis from the study of 95 necropsy patients. Circulation. 1976. 54:140–145.
Article10. Bacchion F, Cukon S, Rizzoli G, Gerosa G, Daliento L, Thiene G, Basso C. Infective endocarditis in bicuspid aortic valve: atrioventricular block as sign of perivalvular abscess. Cardiovasc Pathol. 2007. 16:252–255.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ruptured Subvalvular Aortic Aneurysm of a Person Who Has Bicuspid Aortic Valve
- A Case of Staphylococcal Tricuspid Valve Endocarditis With Para-Aortic Abscess in a Patient With Bicuspid Aortic Valve
- Implantation of a permanent pacemaker through the coronary sinus in a patient who underwent mechanical valve replacement for infective endocarditis with a complete atrioventricular block
- Mitral-aortic Intervalvular Fibrosa Pseudoaneurysm with Dual Fistula and Complete AV Block after Aortic Valve Replacement in a Patients with Infective Endocarditis of Aortic Valve
- Anterior Mitral Leaflat Perforation in Patients with Bicuspid Aortic Valve Endocarditis
