Clin Exp Otorhinolaryngol.
2014 Sep;7(3):229-231. 10.3342/ceo.2014.7.3.229.
Nasal Deformity Due to Tuberculous Chondritis
- Affiliations
-
- 1Department of Infectious Diseases, Kyung Hee University Hospital, Kyung Hee University School of Medicine, Seoul, Korea.
- 2Division of Infectious Diseases, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. krpeck@skku.edu
- KMID: 1973476
- DOI: http://doi.org/10.3342/ceo.2014.7.3.229
Abstract
- Tuberculosis (TB) is a common disease worldwide. However, nasal TB is quite rare, and the diagnosis of nasal TB requires a high index of suspicion. The most common symptoms of this unusual presentation are nasal obstruction and nasal discharge. We present a case of nasal TB with involvement of the hard palate presenting with a chronically progressive nasal deformity and ulceration of the hard palate. A biopsy confirmed the diagnosis, and medication for TB was started and the lesions resolved. When a patient presents with chronic ulcerative lesions that do not respond to antibiotic treatment, TB should be included in the differential diagnosis. Biopsy of the lesion can aid in the confirmation of the diagnosis.
Keyword
MeSH Terms
Figure
-

Fig. 1 Initial physical examination. The patient presented with a nasal deformity with inflammation (A, B) and a chronic ulcerative lesion of the hard palate (C, arrow).
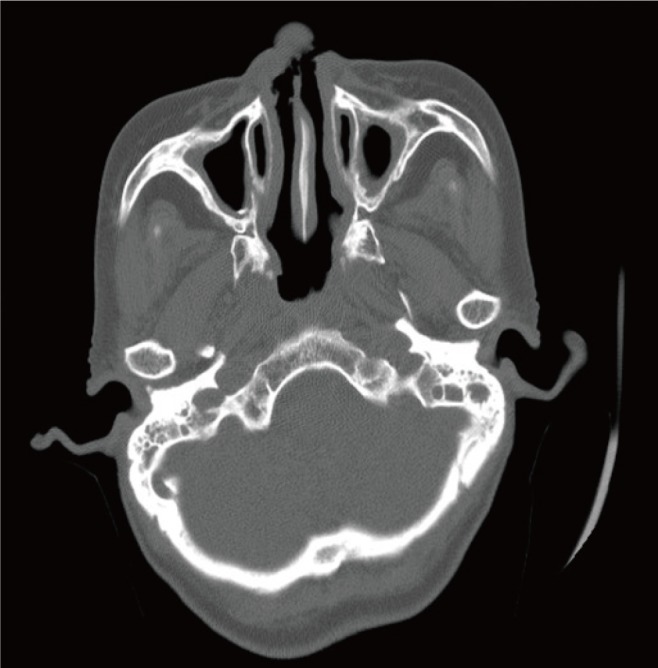
Fig. 2 Computed tomography findings. Perforation of the nasal septum of cartilaginous portion and defect of external nose.
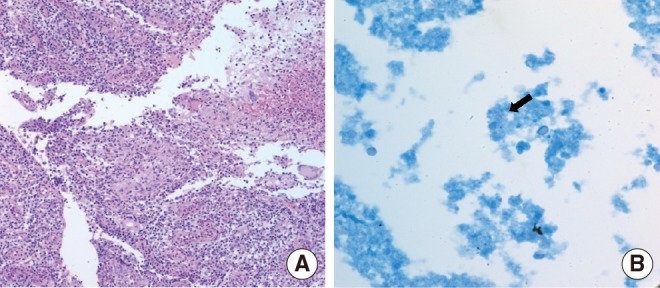
Fig. 3 Histopathology of the nasal tissue. (A) Collections of epithelioid histiocytes forming granulomas and multinucleated giant cells against a necrotic background (H&E, ×100). (B) A few acid-fast bacilli were observed (Ziehl-Neelsen, ×1,000).
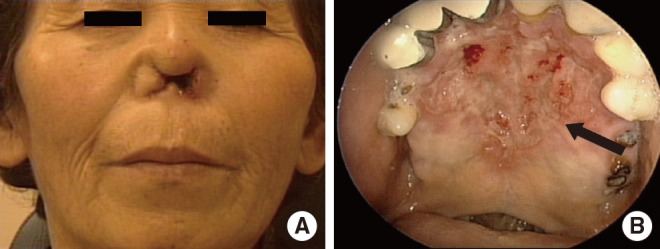
Fig. 4 Follow-up physical examination. Following one year of treatment, the inflammation of the nasal deformity (A) and the chronic ulcerative lesion of the hard palate (B, arrow) both improved.
Reference
-
1. Pust RE. Tuberculosis in the 1990's: resurgence, regimens, and resources. South Med J. 1992; 6. 85(6):584–593. PMID: 1604386.2. Kim YM, Kim AY, Park YH, Kim DH, Rha KS. Eight cases of nasal tuberculosis. Otolaryngol Head Neck Surg. 2007; 9. 137(3):500–504. PMID: 17765784.
Article3. Morgagni GB. On the seats and causes of diseases as investigated by anatomy. Venice. 1761; 1:50–55.4. Butt AA. Nasal tuberculosis in the 20th century. Am J Med Sci. 1997; 6. 313(6):332–335. PMID: 9186146.
Article5. Harries AD, Dye C. Tuberculosis. Ann Trop Med Parasitol. 2006; Jul-Sep. 100(5-6):415–431. PMID: 16899146.6. Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC. Consensus statement. Global burden of tuberculosis: estimated incidence, prevalence, and mortality by country. WHO Global Surveillance and Monitoring Project. JAMA. 1999; 8. 282(7):677–686. PMID: 10517722.7. Goguen LA, Karmody CS. Nasal tuberculosis. Otolaryngol Head Neck Surg. 1995; 7. 113(1):131–135. PMID: 7603707.
Article8. Prasad KC, Sreedharan S, Chakravarthy Y, Prasad SC. Tuberculosis in the head and neck: experience in India. J Laryngol Otol. 2007; 10. 121(10):979–985. PMID: 17367564.
Article9. Lai TY, Liu PJ, Chan LP. Primary nasal tuberculosis presenting with septal perforation. J Formos Med Assoc. 2007; 11. 106(11):953–955. PMID: 18063517.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Three Cases of Relapsing Polychondritis
- Reconstructive rhinoplasty with costal cartilage grafting: A case report of relapsing polychondritis
- Saddle nose deformity caused by CO2 laser vaporization of papillomas from the nasal septum: a case report
- Nasal Deformity and Acoustic Airway Obstruction Profiles in Unilateral Secondary Cleft Lip Nose Deformity
- ANALYSIS OF NASAL TIP PLASTY
