Technical Considerations of Endoscopic Subureteral Injection for the Treatment of Vesicoureteral Reflux
- Affiliations
-
- 1Department of Urology, Guro Hospital, Korea University College of Medicine, Seoul, Korea. dgmoon@korea.ac.kr
- KMID: 1973386
- DOI: http://doi.org/10.4068/cmj.2008.44.1.17
Abstract
- The purpose of this study was to assess the long-term efficacy and the cause of failure in endoscopic subureteral injection for vesicoureteral reflux. For 5 years, a total of 73 patients (96 ureters) with primary grades I to V VUR were treated by one operator using subureteral injection of polydimethylsiloxane (PDS) and followed-up for more than 1 year. Cure was defined as an absence of VUR on voiding cystourethrography at 3 months after injection. Second and third injection was done for the failed cases. Statistical analyses were performed using the chi-square test. Endoscopic subureteral injection of PDS showed high success rate (82.3%) after single injection, 98% after second injection for the failed cases. Correction by grade was 75%, 83%, 89%, 83%, and 77% for grade I to V, respectively. In 17 units of second injection, cystoscopy showed mound displacement in 9 units, no volcano appearance but rather a broad elevation in 5 units, mound extrusion in 2 units, and distal ureteral fistula in 1 unit. Among 17 failed units, 58.8% (10/17) occurred in the first 18 months, meanwhile, failure rate decreased to 9.5% (7/74) in later 42 months during the 5 years' practice in our institute. In contrast to the generally accepted concept, the primary grade was not the main cause of success. Besides the primary reflux grade, available position according to the characteristics of the patients, injection method, the operator's skill and experience greatly affect the success rate.
MeSH Terms
Figure
-
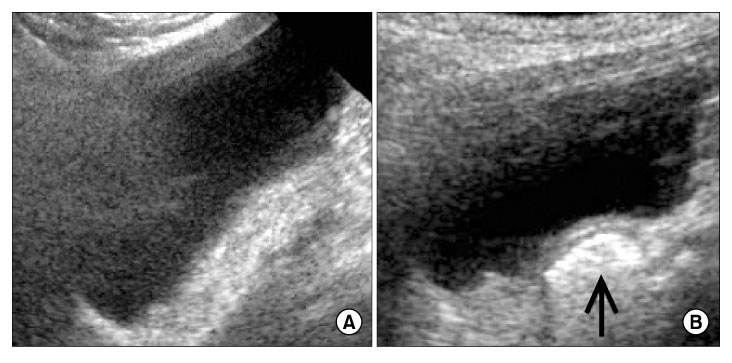
Fig. 1 Sonographic finding of the urinary bladder. (A) No specific echogenic was noted at the right ureteral orifice on preoperative sonography.(B) An echogenic nodule (arrow) of injected PDS is noted on post-operative sonography.
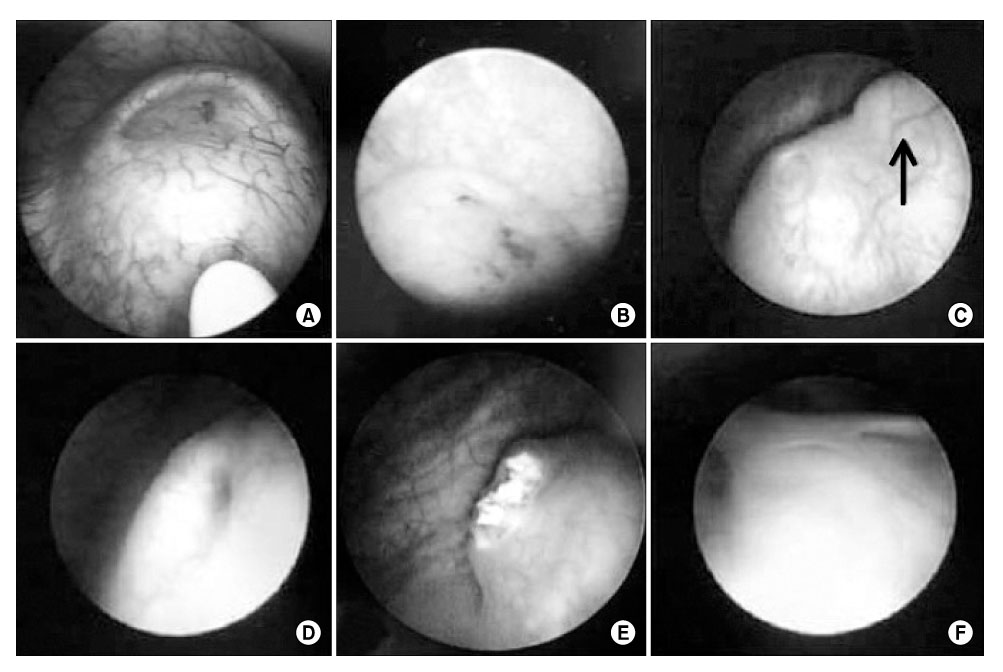
Fig. 2 Operative cystoscopic findings. (A) Creation of competent ureteral orifice by cystoscopic submucosal injection of PDS. (B) Competent ureteral orifice on the top of a 'volcano' after injection of PDS. (C) Incompetent ureteral orifice; a main mound (arrow) is seen above the ureteral orifice. (D) Incompetent ureteral orifice; a mound is still poorly seen around ureteral orifice at 5~7 o'clock. (E) Extrusion of PDS is seen due to mucosal necrosis after overcorrection. (F) Ureteral fistula at the right. ureteral orifice is seen. It might be the result of complete extrusion of PDS after overcorrection.
Reference
-
1. Lavelle MT, Conlin MJ, Skoog SJ. Subureteral injection of deflux for correction of reflux: analysis of factors predicting success. Urology. 2005. 65:564–567.
Article2. Perez-Brayfield M, Kirsch AJ, Hensle TW, Koyle MA, Furness P, Scherz HC. Endoscopic treatment with dextranomer/hyaluronic acid for complex cases of vesicoureteral reflux. J Urol. 2004. 172:1614–1616.
Article3. Kirsch AJ, Perez-Brayfield MR, Scherz HC. Minimally invasive treatment of vesicoureteral reflux with endoscopic injection of dextranomer/ hyaluronic acid copolymer: the Children's Hospitals of Atlanta experience. J Urol. 2003. 170:211–215.
Article4. Kirsch AJ, Perez-Brayfield M, Smith EA, Scherz HC. The modified sting procedure to correct vesicoureteral reflux: improved results with submucosal implantation within the intramural ureter. J Urol. 2004. 171:2413–2416.
Article5. Aboutaleb H, Bolduc S, Khoury AE, Upadhyay J, Bägli DJ, Farhat W. Polydimethylsiloxane injection versus open surgery for the treatment of vesicoureteral reflux in complete duplex systems. J Urol. 2003. 170:1563–1565.
Article6. Herz D, Hafez A, Bagli D, Capolicchio G, McLorie G, Khoury A. Efficacy of endoscopic subureteral polydimethylsiloxane injection for treatment of vesicoureteral reflux in children: a North American clinical report. J Urol. 2001. 166:1880–1886.
Article7. Aboutaleb H, Bolduc S, Upadhyay J, Farhat W, Bägli DJ, Khoury AE. Subureteral polydimethylsiloxane injection versus extravesical reimplantation for primary low grade vesicoureteral reflux in children: a comparative study. J Urol. 2003. 169:313–316.
Article8. Vandersteen DR, Routh JC, Kirsch AJ, Scherz HC, Ritchey ML, Shapiro E, et al. Postoperative ureteral obstruction after subureteral injection of dextranomer/hyaluronic acid copolymer. J Urol. 2006. 176:1593–1595.
Article9. Joyner BD, Atala A. Endoscopic substances for the treatment of vesicoureteral reflux. Urology. 1997. 50:489–494.
Article10. Higham-Kessler J, Reinert SE, Snodgrass WT, Hensle TW, Koyle MA, Hurwitz RS, et al. A review of failures of endoscopic treatment of vesicoureteral reflux with dextranomer microspheres. J Urol. 2007. 177:710–714.
Article11. Capozza N, Lais A, Matarazzo E, Nappo S, Patricolo M, Caione P. Influence of voiding dysfunction on the outcome of endoscopic treatment for vesicoureteral reflux. J Urol. 2002. 168:1695–1698.
Article12. Menezes MN, Puri P. The role of endoscopic treatment in the management of grade v primary vesicoureteral reflux. Eur Urol. 2007. 52:1505–1509.
Article13. Capozza N, Lais A, Nappo S, Caione P. The role of endoscopic treatment of vesicoureteral reflux: a 17-year experience. J Urol. 2004. 172:1626–1628.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Early Experience and Technical Aspects of Endoscopic Subureteral Polydimethylsiloxane Injection for Vesicoureteral Reflux
- Endoscopic teflon injection in vesicoureteral reflux
- Experience of Subureteral Polydimethylsiloxane Injection Treatment in Children with Vesicoureteral Reflux
- Effect of Subureteral Injection of Polydimethylsiloxane in Women with Vesicoureteral Reflux
- An Experience of Endoscopic Polydimethylsiloxane Injection for the Treatment of Vesicoureteral Reflux in Children
