Korean Circ J.
2015 Jul;45(4):333-336. 10.4070/kcj.2015.45.4.333.
Constrictive Pericarditis Long after a Gunshot Wound
- Affiliations
-
- 1Department of Cardiology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. mhlee@yuhs.ac
- 2Department of Radiology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Cardiovascular Surgery, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1964106
- DOI: http://doi.org/10.4070/kcj.2015.45.4.333
Abstract
- Constrictive pericarditis is an uncommon post-inflammatory disorder characterized by a variably thickened, fibrotic, and frequently calcified, pericardium. Etiology of the constriction can occur for many reasons. Although foreign bodies are not the common cause of constrictive pericarditis, the long-term presence of foreign bodies, like bullets, is presumed to cause chronic constrictive pericarditis even after a very long asymptomatic period. A 69-year-old patient with atrial flutter was admitted to the hospital. A cardiac computed tomography showed a bullet located adjacent to the right atrium. The transthoracic echocardiography showed a thickened pericardium and septal bouncing motion, which were compatible with constrictive pericarditis. The history of the patient revealed an injury by gunshot during the Korean War in 1950. Radiofrequency ablation of the atrial flutter was performed, and after ablation, the bullet was removed surgically. The patient was discharged home after surgery without complications.
MeSH Terms
Figure
-

Fig. 1 Chest X-ray shows a bullet adjacent to the right cardiac border and bilateral pleural effusion.
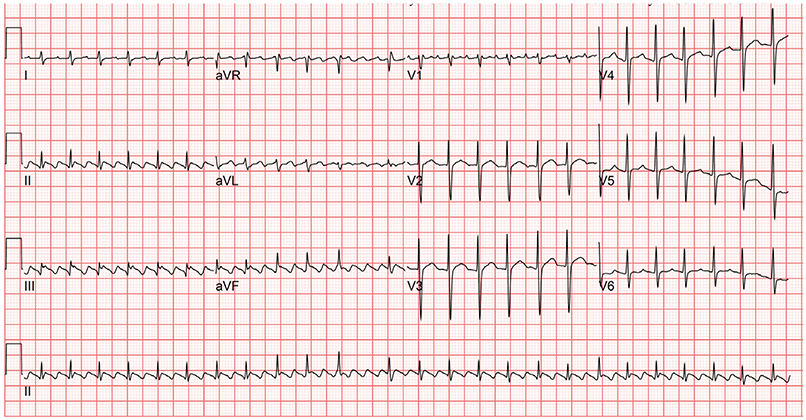
Fig. 2 Electrocardiography shows a typical atrial flutter with 2-to-1 atrioventricular conduction.

Fig. 3 Computed tomographic images confirm that the bullet is located in the epicardial fat. A: axial image. B: long axis image. C: three-dimensional volume-rendered image.
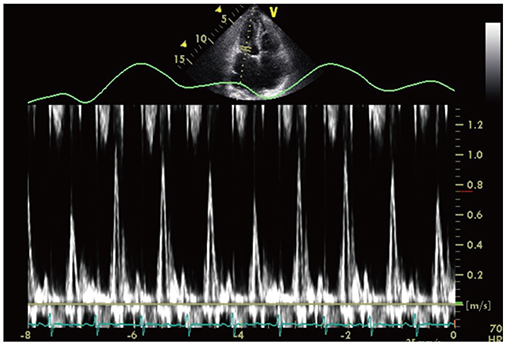
Fig. 4 Pulsed-wave Doppler image reveals significant respiratory variation of the mitral inflow velocity.

Fig. 5 The bullet (arrow) in the surgical field.

Fig. 6 Hyalinized degeneration (arrows) of the pericardial tissue (hematoxylin-eosin stain, ×100).
Reference
-
1. Myers RB, Spodick DH. Constrictive pericarditis: clinical and pathophysiologic characteristics. Am Heart J. 1999; 138(2 Pt 1):219–232.2. Ling LH, Oh JK, Schaff HV, et al. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy. Circulation. 1999; 100:1380–1386.3. Meyns BP, Faveere BC, Van de Werf FJ, Dotremont G, Daenen WJ. Constrictive pericarditis due to ingestion of a toothpick. Ann Thorac Surg. 1994; 57:489–490.4. LeMaire SA, Wall MJ Jr, Mattox KL. Needle embolus causing cardiac puncture and chronic constrictive pericarditis. Ann Thorac Surg. 1998; 65:1786–1787.5. Wood P. Chronic constrictive pericarditis. Am J Cardiol. 1961; 7:48–61.6. Dressler W. The post-myocardial-infarction syndrome: a report on forty-four cases. AMA Arch Intern Med. 1959; 103:28–42.7. Monsuez JJ, Deland E, Rabbat A, et al. Constrictive pericarditis developing forty-five years after gunshot wound. J Thorac Cardiovasc Surg. 1992; 104:846–848.8. LiMandri G, Gorenstein LA, Starr JP, Homma S, Auteri J, Gopal AS. Use of transesophageal echocardiography in the detection and consequences of an intracardiac bullet. Am J Emerg Med. 1994; 12:105–106.9. Burkhart HM, Gomez GA, Jacobson LE, Broadie TA, Tarver RD. Meandering bullet in the pericardial sac: to remove or not to remove. Am Surg. 1998; 64:341–343.10. Talreja DR, Edwards WD, Danielson GK, et al. Constrictive pericarditis in 26 patients with histologically normal pericardial thickness. Circulation. 2003; 108:1852–1857.11. Davis RE, Bruno AD 2nd, Larsen WB, Sugimoto JT, Gaines RD. Mobile intrapericardial bullet: case report and review of the literature. J Trauma. 2005; 58:378–380.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Constrictive Pericarditis Following Acute Idiopathic Pericarditis
- Echocardiographic Evaluation of Constrictive Pericarditis
- Tuberculous Constrictive Pericarditis: A Classical Case and Review
- Constrictive Pericarditis as a Never Ending Story: What's New?
- A Case of Constrictive Pericarditis with Localized Pericardial Effusion Simulating a Cystic Mass
