Iatrogenic Carotid-Cavernous Fistula after Stent Assisted Coil Embolization of Posterior Communicating Artery Aneurysm
- Affiliations
-
- 1Department of Neurosurgery, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. smyoon@sch.ac.kr
- KMID: 1963149
- DOI: http://doi.org/10.7461/jcen.2015.17.1.43
Abstract
- Stent assisted coiling (SAC) is a useful technique for the treatment of wide necked complex aneurysm. As the frequency of SAC increases, stent-related complications such as thromboembolism, aneurysm rupture, and vessel rupture have been reported. However, to the best of our knowledge, carotid-cavernous fistula (CCF) after SAC has never been reported. The authors experienced a case of direct CCF after a SAC procedure for treatment of a complex posterior communicating artery (PCoA) aneurysm regrowth, which was treated by clip ligation 12 years before. The patient was managed conservatively and angiograms performed three months after the procedure showed the complete obliteration of the left PcoA aneurysm and the spontaneous disappearance of CCF. Navigation of Solitaire stent lumen with microcatheter can cause unexpected arterial injury, especially when the proximal tip is placed in the curved portion. It seems to be desirable to place the proximal tip of Solitaire stent in the straight portion whenever possible to reduce the risk of inadvertent arterial injury which might be caused by future navigation of stent lumen.
MeSH Terms
Figure
-
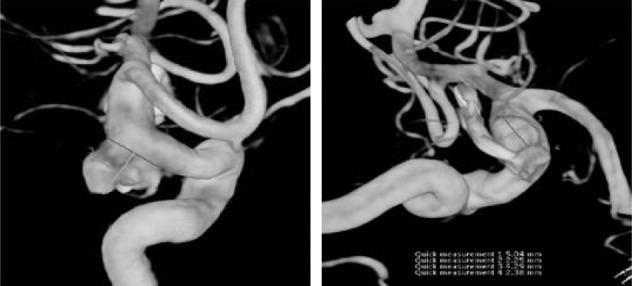
Fig. 1 A cerebral angiogram revealed a posteromedially regrowing, irregularly shaped posterior communicating artery (PCoA) aneurysm, with a neck size of 7.22 mm and a dome size of 7.3 × 5.2 mm. The origin of a small PCoA was incorporated in the aneurysmal neck.
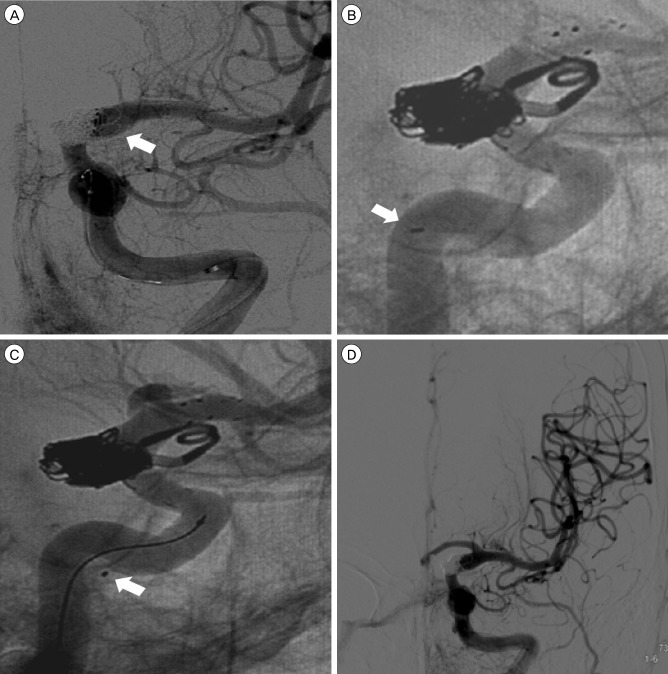
Fig. 2 After packing eight coils, it became difficult to verify whether the internal carotid artery (ICA) lumen was compromised by coils (A). Before carotid-cavernous fistula (CCF) occurrence, the proximal tip of the Solitaire stent was located within the ICA lumen (B). Shortly after CCF occurrence, the authors identified the proximal tip of the Solitaire stent beyond the confines of the ICA lumen (C). The procedure was stopped after complete obliteration of the aneurysm without compromising ICA and middle cerebral artery flow, while the CCF remained (D).

Fig. 3 A follow-up angiogram seven days after the procedure. A high-flow carotid-cavernous fistula (CCF) was still visible without the cortical venous reflux (A). After conservative management, angiograms from three months after the procedure showed the complete obliteration of the left posterior communicating artery aneurysm and the spontaneous disappearance of CCF (B).
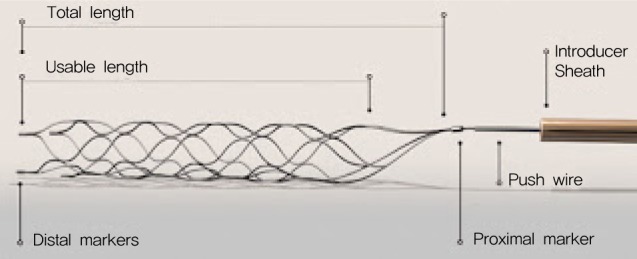
Fig. 4 The structure of the Solitaire stent. The stent system consists of an attached firm push wire that enables the deployment and retrieval of the device. Although the Solitaire stent is known to be highly flexible, the proximal tip component cannot be flexible due to its structural nature.
Reference
-
1. Akpek S, Arat A, Morsi H, Klucznick RP, Strother CM, Mawad ME. Self-expandable stent-assisted coiling of wide-necked intracranial aneurysms: a single-center experience. AJNR Am J Neuroradiol. 2005; 5. 26(5):1223–1231. PMID: 15891189.2. Amagasaki K, Higa T, Takeuchi N, Kakizawa T, Shimizu T. Late recurrence of subarachnoid hemorrhage due to regrowth of aneurysm after neck clipping surgery. Neurol Med Chir (Tokyo). 002; 11. 42(11):496–500. PMID: 12472214.3. Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985; 2. 62(2):248–256. PMID: 3968564.
Article4. Benndorf G, Bender A, Lehmann R, Lanksch W. Transvenous occlusion of dural cavernous sinus fistulas through the thrombosed inferior petrosal sinus: report of four cases and review of the literature. Surg Neurol. 2000; 7. 54(1):42–54. PMID: 11024506.
Article5. Biondi A, Milea D, Cognard C, Ricciardi GK, Bonneville F, van Effenterre R. Cavernous sinus dural fistulae treated by transvenous approach through the facial vein: report of seven cases and review of the literature. AJNR Am J Neuroradiol. 2003; Jun-Jul. 24(6):1240–1246. PMID: 12812963.6. Bujak M, Margolin E, Thompson A, Trobe JD. Spontaneous resolution of two dural carotid-cavernous fistulas presenting with optic neuropathy and marked congestive ophthalmopathy. J Neuroophthalmol. 2010; 9. 30(3):222–227. PMID: 20498622.
Article7. Cekirge H, Islak C, Firat M, Kocer N, Saatci I. Endovascular coil embolization of residual or recurrent aneurysms after surgical clipping. Acta Radiol. 2000; 3. 41(2):111–115. PMID: 10741780.
Article8. Giannotta SL, Litofsky NS. Reoperative management of intracranial aneurysms. J Neurosurg. 1995; 9. 83(3):387–393. PMID: 7666212.
Article9. Gupta AK, Purkayastha S, Krishnamoorthy T, Bodhey NK, Kapilamoorthy T, Kesavadas C, et al. Endovascular treatment of direct carotid cavernous fistulae: a pictorial review. Neuroradiology. 2006; 11. 48(11):831–839. PMID: 16969673.
Article10. Horowitz M, Levy E, Sauvageau E, Genevro J, Guterman LR, Hanel R, et al. Intra/extra-aneurysmal stent placement for management of complex and wide-necked-bifurcation aneurysms: eight cases using the waffle cone technique. Neurosurgery. 2006; 4. 58(4 Suppl 2):ONS-258-62.11. Kanamalla US, Jungreis CA, Kochan JP. Direct carotid cavernous fistula. In : Hurst RW, Rosenwasser RH, editors. Interventional Neuroradiology. New York: Informa healthcare;2008. p. 231–238.12. Klisch J, Eger C, Sychra V, Strasilla C, Basche S, Weber J. Stent-Assisted Coil Embolization of Posterior Circulation Aneurysms Using Solitaire Ab: Preliminary Experience. Neurosurgery. 2009; 8. 65(2):258–266. PMID: 19625903.13. Kwon HJ, Jin SC. Spontaneous healing of iatrogenic direct carotid cavernous fistula. Interv Neuroradiol. 2012; 6. 18(2):187–190. PMID: 22681734.
Article14. Lanzino G, Wakhloo AK, Fessler RD, Hartney ML, Guterman LR, Hopkins LN. Efficacy and current limitations of intravascular stents for intracranial internal carotid, vertebral, and basilar artery aneurysms. J Neurosurg. 1999; 10. 91(4):538–546. PMID: 10507372.
Article15. Lee YJ, Kim DJ, Suh SH, Lee SK, Kim J, Kim DI. Stent-assisted coil embolization of intracranial wide-necked aneurysms. Neuroradiology. 2005; 9. 47(9):680–689. PMID: 16028036.
Article16. Liebig T, Henkes H, Reinartz J, Miloslavski E, Kühne D. A novel self-expanding fully retrievable intracranial stent (SOLO): experience in nine procedures of stent-assisted aneurysm coil occlusion. Neuroradiology. 2006; 7. 48(7):471–478. PMID: 16758153.
Article17. Nishijima M, Iwai R, Horie Y, Oka N, Takaku A. Spontaneous occlusion of traumatic carotid cavernous fistula after orbital venography. Surg Neurol. 1985; 5. 23(5):489–492. PMID: 3983805.
Article18. Park HR, Yoon SM, Shim JJ, Kim SH. Waffle-cone technique using Solitaire AB stent. J Korean Neurosurg Soc. 2012; 4. 51(4):222–226. PMID: 22737303.
Article19. Rabinstein AA, Nichols DA. Endovascular coil embolization of cerebral aneurysm remnants after incomplete surgical obliteration. Stroke. 2002; 7. 33(7):1809–1815. PMID: 12105358.
Article20. Rahal JP, Dandamudi VS, Safain MG, Malek AM. Double waffle-cone technique using twin Solitaire detachable stents for treatment of an ultra-wide necked aneurysm. J Clin Neurosci. 2013; 6. 21(6):1019–1023. PMID: 24412295.
Article21. Reider-Grosswasser I, Loewenstein A, Gaton DD, Lazar M. Spontaneous thrombosis of a traumatic cavernous sinus fistula. Brain Inj. 1993; 11. 7(6):547–550. PMID: 8260959.
Article22. Sluzewski M, Van Rooij WJ, Beute GN, Nijssen PC. Balloon-assisted coil embolization of intracranial aneurysms: incidence, complications, and angiography results. J Neurosurg. 2006; 9. 105(3):396–399. PMID: 16961133.
Article23. Sychra V, Klisch J, Werner M, Dettenborn C, Petrovitch A, Strasilla C, et al. Waffle-cone technique with Solitaire™ AB Remodeling Device: endovascular treatment of highly selected complex cerebral aneurysms. Neuroradiology. 2011; 12. 53(12):961–972. PMID: 20821314.
Article24. Tjoumakaris SI, Jabbour PM, Rosenwasser RH. Neuroendovascular management of carotid cavernous fistulae. Neurosurg Clin N Am. 2009; 10. 20(4):447–452. PMID: 19853804.
Article25. Vanninen R, Manninen H, Ronkainen A. Broad-based intracranial aneurysms: thrombosis induced by stent placement. AJNR Am J Neuroradiol. 2003; 2. 24(2):263–266. PMID: 12591645.26. Voigt K, Sauer M, Dichgans J. Spontaneous occlusion of a bilateral caroticocavernous fistula studied by serial angiography. Neuroradiology. 1971; 9. 2(4):207–211. PMID: 5164129.
Article27. Wanke I, Doerfler A, Schoch B, Stolke D, Forsting M. Treatment of wide-necked intracranial aneurysms with a self-expanding stent system: initial clinical experience. AJNR Am J Neuroradiol. 2003; Jun-Jul. 24(6):1192–1199. PMID: 12812954.28. Wanke I, Forsting M. Stents for intracranial wide-necked aneurysms: more than mechanical protection. Neuroradiology. 2008; 12. 50(12):991–998. PMID: 18807024.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Retrograde Stent-assisted Coil Embolization of Wide-neck or Branch-incorporated Posterior Communicating Artery Aneurysm
- Persistent Trigeminal Artery with a Cerebellar Branch and Trigeminal-Cavernous Fistula from Ruptured Aneurysm: Transarterial Coil Embolization
- Traumatic Carotid Cavernous Fistula Caused by Intradural Aneurysm Rupture: A Case Report
- Dual Stent-Assisted Coil Embolization for Fusiform Aneurysm Arising From Persistent Trigeminal Artery
- GDC(Guglielmi Detachable Coil) Embolization Used in Carotid-Cavernous Fistula Incompletely Occluded by Detachable Balloon
