Regrowth of Cervical Intradural Lipoma without Spinal Dysraphism
- Affiliations
-
- 1Department of Neurosurgery, Pusan National University Yangsan Hospital, Yangsan, Korea. md6576@naver.com
- 2Department of Neurosurgery, Pusan National University Hospital, Busan, Korea.
- KMID: 1956521
- DOI: http://doi.org/10.3340/jkns.2014.56.2.157
Abstract
- A 49 years old male patient who suffered from deterioration of posterior neck pain, left hand numbness, left lower limb pain and gait disturbance for 3 years visited our outpatient department. He had been diagnosed as non-dysraphic cervical intradural lipoma and operated in August 1990. On the radiologic images, we found the regrowth of non-dysraphic cervical intradural lipoma from C2 to C7 level, which surrounds and compresses the cervical spinal cord. Previous subtotal laminectomy from C2 to C7 and severe cervical lordosis were also found. Appropriate debulking of lipoma mass without duroplasty was successfully done with intraoperative neurophysiological monitoring (IONM). We are following up the patient for 24 months via outpatient department, his neurologic symptoms such as hand numbness, gait disturbance, left lower limb pain and posterior neck pain have improved. We describe a rare case of regrowth of non-dysraphic cervical intradural lipoma.
MeSH Terms
Figure
-
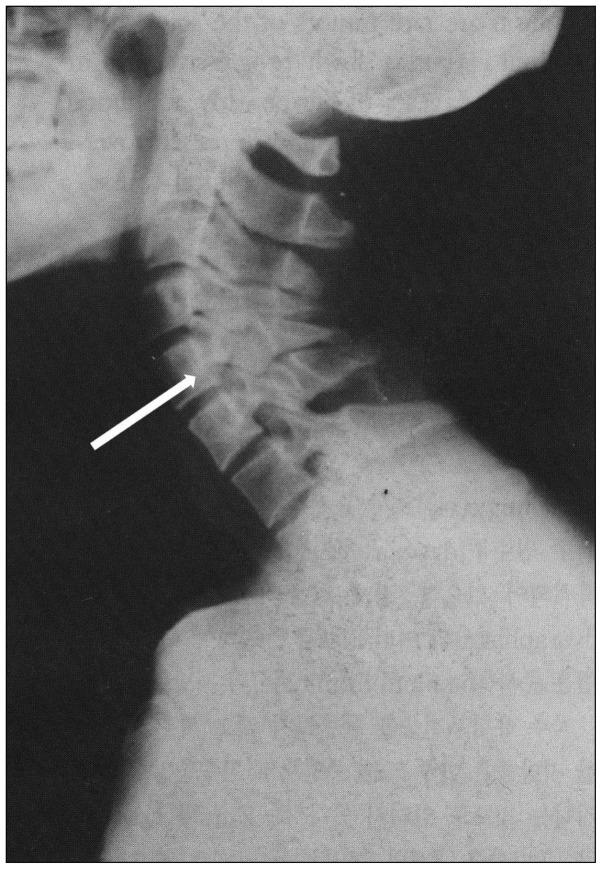
Fig. 1 Preoperative cervical plain film at the time of the first operation shows severe cervical lordosis and increased anteroposterior diameter of the spinal canal (arrow), which may suggest the presence of a mass lesion in the vertebral canal.

Fig. 2 Preoperative CT image at the time of the first operation shows a hypodense tumor mass occupying the spinal canal almost entirely. Cervical spinal cord was severely compressed and located peripherally in the spinal canal.

Fig. 3 Preoperative T1-weighted sagittal image at the time of the first operation shows a huge intradural mass with high signal intensity located from the C2 to C7 level. Axial image shows that this mass occupies the entire spinal canal and distorts the cervical spinal cord.
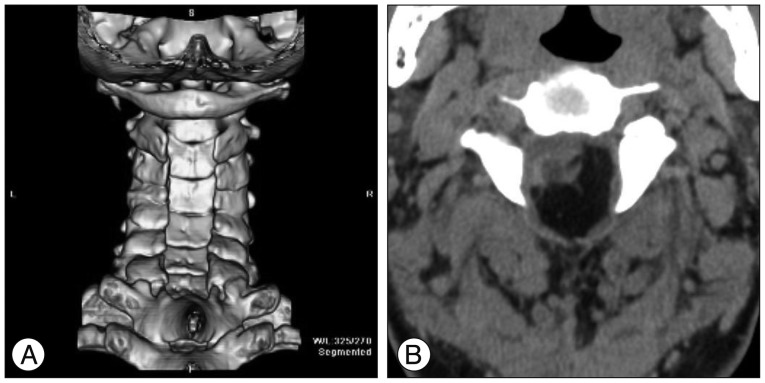
Fig. 4 Preoperative 3-dimensional CT images at the time of the second operation show previous subtotal laminectomy from C2 to C7 (A). The hypodense intradural mass is the recurred intradural lipoma, and it also compresses and distorts the cervical spinal cord (B).

Fig. 5 Preoperative T1- (A) and T2- (B) weighted MRI images at the time of the second operation show an intradural lipoma from the C2 to C7 level exhibiting high signal intensity, suggesting a regrown lipomatous mass.
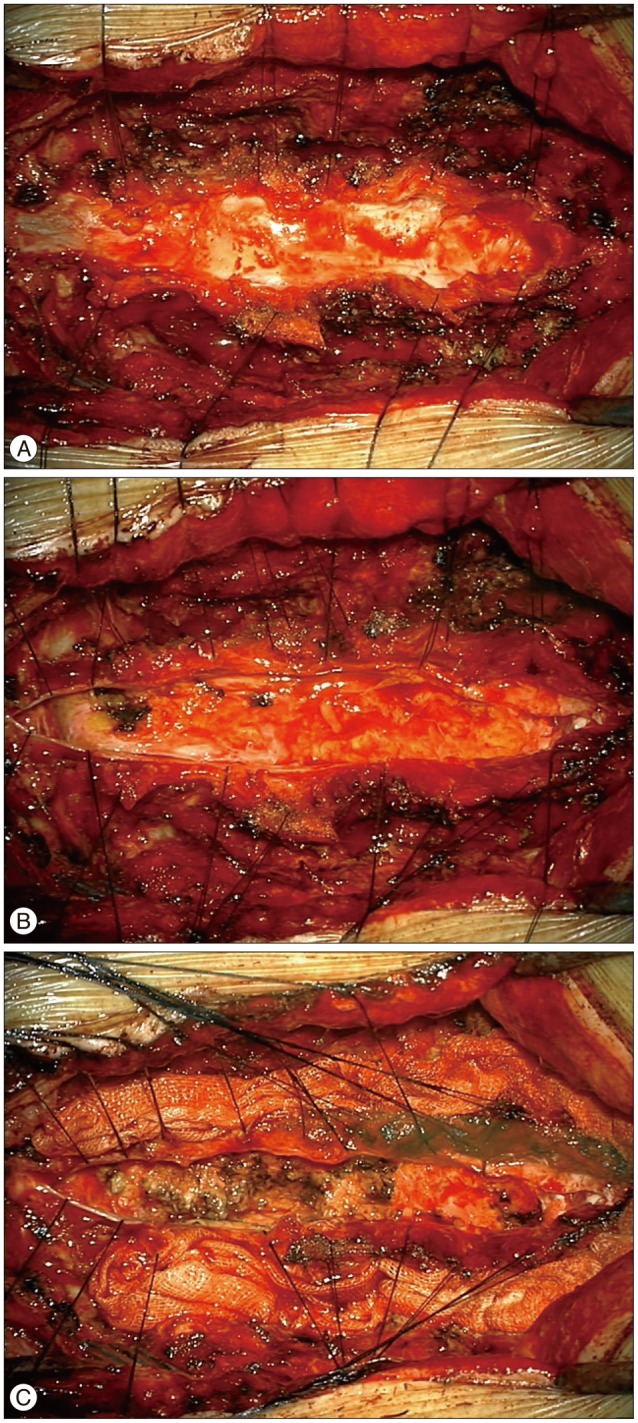
Fig. 6 During the operation, there were severe adhesions between the cervical dura, paraspinal muscles and soft tissues. A : When we incised the cervical dura after performing dissection of adhesions, we found a huge, yellowish mass in the intradural space, and it looked like a lipomatous mass. B : After performing subtotal debulking of the lipomatous mass, we achieved adequate decompression of the spinal canal. C : Thus, we could close the cervical dura without duraplasty.
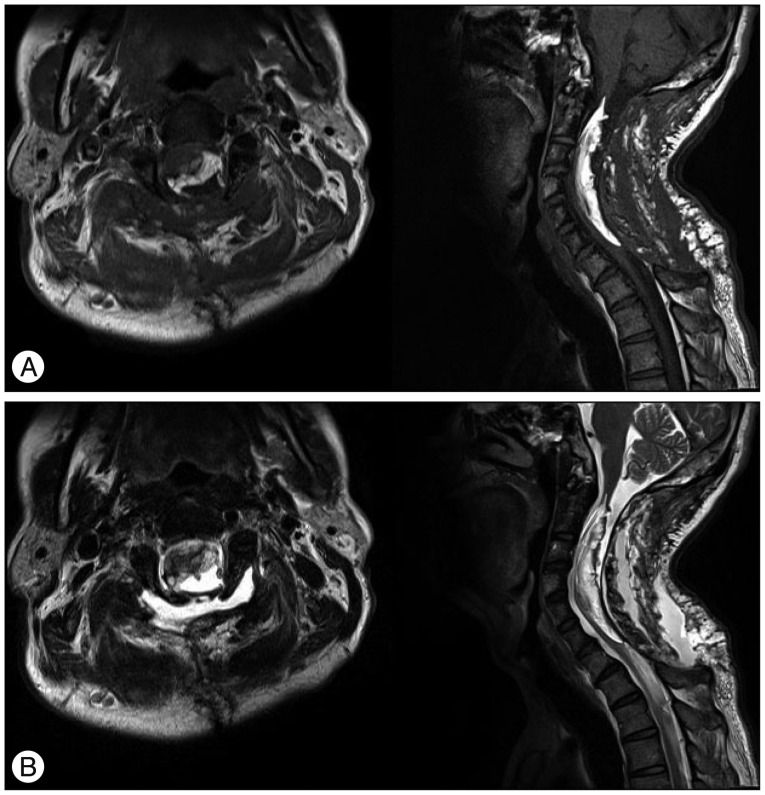
Fig. 7 Postoperative T1- (A) and T2- (B) weighted MRI images show that the debulked intradural lipoma at the C2-7 vertebral level exhibits high signal intensity. The low signal intensity mass on T1-weighted image and the high signal intensity mass on T2-weighted image suggest fluid collection at the surgical site, it was found to be cerebrospinal fluid.

Fig. 8 Peripherally located nucleus and vacant cytoplasm without fat necrosis confirm the presence of mature adipose cells, suggesting the diagnosis of lipoma (Hematoxylin and Eosin stain, ×200).
Reference
-
1. Akyuz M, Goksu E, Tuncer R. Spontaneous decrease in the size of a residual thoracic intradural lipoma. Br J Neurosurg. 2005; 19:53–55. PMID: 16156032.
Article2. Bhatoe HS, Singh P, Chaturvedi A, Sahai K, Dutta V, Sahoo PK. Nondysraphic intramedullary spinal cord lipomas : a review. Neurosurg Focus. 2005; 18:ECP1. PMID: 15715454.4. Caram PC, Carton CA, Scarcella G. Intradural lipomas of the spinal cord; with particular emphasis on the intramedullary lipomas. J Neurosurg. 1957; 14:28–42. PMID: 13385701.5. Elsberg CA. Some aspects of the diagnosis and surgical treatment of tumors of the spinal cord : with a study of the end results in a series of 119 operations. Ann Surg. 1925; 81:1057–1073. PMID: 17865272.
Article6. Fleming KL, Davidson L, Gonzalez-Gomez I, McComb JG. Nondysraphic pediatric intramedullary spinal cord lipomas : report of 5 cases. J Neurosurg Pediatr. 2010; 5:172–178. PMID: 20121366.7. Fujiwara F, Tamaki N, Nagashima T, Nakamura M. Intradural spinal lipomas not associated with spinal dysraphism : a report of four cases. Neurosurgery. 1995; 37:1212–1215. PMID: 8584165.8. Giuffrè R. Intradural spinal lipomas. Review of the literature (99 cases) and report of an additional case. Acta Neurochir (Wien). 1966; 14:69–95. PMID: 5972947.9. Iwatsuki K. Intradural cervical lipoma with parenchymal marginal fibrous tissue : case report. Neurosurgery. 2006; 59:E208. discussion E208. PMID: 16823291.10. Kabir SM, Thompson D, Rezajooi K, Casey AT. Non-dysraphic intradural spinal cord lipoma : case series, literature review and guidelines for management. Acta Neurochir (Wien). 2010; 152:1139–1144. PMID: 20221647.
Article11. Kim CH, Wang KC, Kim SK, Chung YN, Choi YL, Chi JG, et al. Spinal intramedullary lipoma : report of three cases. Spinal Cord. 2003; 41:310–315. PMID: 12714995.12. Klekamp J, Fusco M, Samii M. Thoracic intradural extramedullary lipomas. Report of three cases and review of the literature. Acta Neurochir (Wien). 2001; 143:767–773. discussion 773-774. PMID: 11678397.
Article13. McGillicuddy GT, Shucart W, Kwan ES. Intradural spinal lipomas. Neurosurgery. 1987; 21:343–346. PMID: 3670579.
Article14. O'Grady J, Kaliaperumal C, O'Sullivan M. Recurrent 'universal tumour' of the spinal cord. BMJ Case Rep. 2012; doi : 10.1136/bcr.12.2011.5284.15. Park IS, Choi CH, Lee YW, Song GS, Park DJ, Cha SH. Huge cervical intradural lipoma in a neurologically intact patient : case report. J Korean Neurosurg Soc. 1995; 24:1583–1589.16. Pruthi N, Devi BI. Nondysraphic cervical and thoracic intraspinal lipomas : a review. Br J Neurosurg. 2010; 24:228–232. PMID: 20465452.
