J Korean Soc Transplant.
2014 Dec;28(4):246-249. 10.4285/jkstn.2014.28.4.246.
Papillary Adenoma Identified in Removed Polycystic Kidneys during Kidney Transplantation in Autosomal Dominant Polycystic Kidney Disease Patient
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea. kidney77@yonsei.ac.kr
- 2Department of Surgery, Yonsei University Wonju College of Medicine, Wonju, Korea.
- 3Department of Pathology, Yonsei University Wonju College of Medicine, Wonju, Korea.
- KMID: 1941321
- DOI: http://doi.org/10.4285/jkstn.2014.28.4.246
Abstract
- Kidney transplantation is the preferred treatment in end stage renal disease for autosomal dominant polycystic kidney disease (ADPKD) patients. Removal of the native kidney is not usually recommended for ADPKD patients during a transplantation procedure because the operation time may be prolonged or the risk of bleeding may be higher. Therefore, native kidney removal is indicated for patients with chronic pain by enlarged kidney, frequent complications from cysts, such as infection or bleeding, and renal tumor development. Here, we report a case of a patient whose native kidneys were removed during a kidney transplantation procedure, and multifocal adenomas were identified in the removed kidneys after the procedure.
MeSH Terms
Figure
-
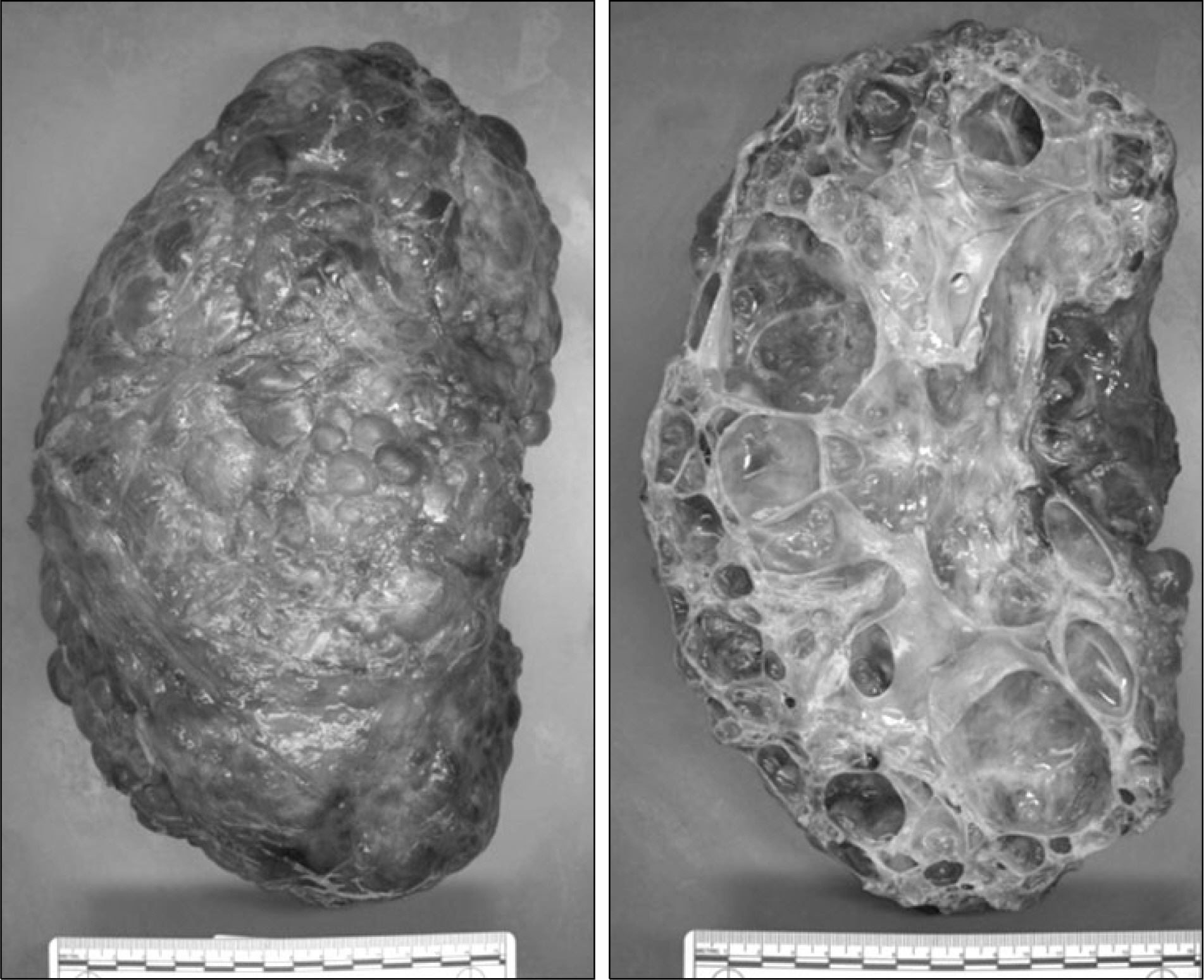
Fig. 1. Gross appearance of polycystic kidney removed from recipient during kidney transplant procedure. The surface and internal part of polycystic kidney are composed of numerous cysts of variable sizes.

Fig. 2. Pathologic findings in the parenchyma of polycystic kidney. (A∼ C) Light microscopy shows papillary proliferation of bland epithelial cells (HE stain, ×200). (D) Immunohistochemical stain for cytokeratin-7 is positive in the cytoplasm of tumor cells (×200).
Reference
-
References
1). Bennett WM. Peritransplant management of retained native kidneys in autosomal dominant polycystic kidney disease. Nephrol Dial Transplant. 2013; 28:245–6.
Article2). Wang KL, Weinrach DM, Luan C, Han M, Lin F, Teh BT, et al. Renal papillary adenoma: a putative precursor of papillary renal cell carcinoma. Hum Pathol. 2007; 38:239–46.3). Zanollo A. [Papillary cystadenoma in the polycystic kidney and papilliferous adenoma in the kidney with diffuse caseous tuberculosis]. Arch Ital Urol. 1966; 38:103–23.4). Finkel LI, Lanesky JR Jr, Taras RJ. Solitary renal adenoma in apolycystic kidney: a unique case. J Am Osteopath Assoc. 1983; 82:564–6.5). Ma SK, Kim SS, Kim SW. Renal papillary adenoma in autosomal dominant polycystic kidney disease. Iran J Kidney Dis. 2013; 7:439.6). Gregoire JR, Torres VE, Holley KE, Farrow GM. Renal epithelial hyperplastic and neoplastic proliferation in autosomal dominant polycystic kidney disease. Am J Kidney Dis. 1987; 9:27–38.
Article7). Chang YL, Chung HJ, Chen KK. Bilateral renal cell carcinoma in a patient with autosomal dominant polycystic kidney disease. J Chin Med Assoc. 2007; 70:403–5.
Article8). Park DJ, Park JH, Lee JE, Seong EY, Joo KW, Kim YS, et al. Multilocular cystic renal cell carcinoma accompanied by autosomal dominant polycytstic kidney disease. Korean J Nephrol. 2005; 24:626–30.9). Keith DS, Torres VE, King BF, Zincki H, Farrow GM. Renal cell carcinoma in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1994; 4:1661–9.
Article10). Hajj P, Ferlicot S, Massoud W, Awad A, Hammoudi Y, Charpentier B, et al. Prevalence of renal cell carcinoma in patients with autosomal dominant polycystic kidney disease and chronic renal failure. Urology. 2009; 74:631–4.
Article11). DeLong MJ, Schmitt D, Scott KM, Ramakumar S, Lien YH. Multicentric papillary renal carcinoma in renal allograft. Am J Kidney Dis. 2003; 42:381–4.
Article12). Filocamo MT, Zanazzi M, Li Marzi V, Guidoni L, Villari D, Dattolo E, et al. Renal cell carcinoma of native kidney after renal transplantation: clinical relevance of early detection. Transplant Proc. 2009; 41:4197–201.
Article13). Ianhez LE, Lucon M, Nahas WC, Sabbaga E, Saldanha LB, Lucon AM, et al. Renal cell carcinoma in renal transplant patients. Urology. 2007; 69:462–4.
Article14). Jung YT, Lee JJ, Lee SH, Lee AL, Huh KH, Kim MS, et al. Clinical characteristics and risk factors for renal cell carcinoma after kidney transplantation. J Korean Soc Transplant. 2013; 27:121–7.
Article15). Misumi T, Ide K, Onoe T, Banshodani M, Tazawa H, Teraoka Y, et al. Incidental renal cell carcinoma presenting in a renal transplant recipient with autosomal dominant polycystic kidney disease: a case report. J Med Case Rep. 2012; 6:154.
Article16). Glassman DT, Nipkow L, Bartlett ST, Jacobs SC. Bilateral nephrectomy with concomitant renal graft transplantation for autosomal dominant polycystic kidney disease. J Urol. 2000; 164(3 Pt 1):661–4.
Article17). Fuller TF, Brennan TV, Feng S, Kang SM, Stock PG, Freise CE. End stage polycystic kidney disease: indications and timing of native nephrectomy relative to kidney transplantation. J Urol. 2005; 174:2284–8.
Article18). Tabibi A, Simforoosh N, Abadpour P, Gholamrezaie HR, Nafar M. Concomitant nephrectomy of massively enlarged kidneys and renal transplantation in autosomal dominant polycystic kidney disease. Transplant Proc. 2005; 37:2939–40.
Article19). Hong J, Kim SJ, Lee SK, Joh JW, Kwon CH, Choi GS, et al. Sequential vs. simultaneous bilateral native nephrectomy and renal transplantation for autosomal dominant polycystic kidney disease. J Korean Soc Transplant. 2008; 22:248–53.20). Kramer A, Sausville J, Haririan A, Bartlett S, Cooper M, Phelan M. Simultaneous bilateral native nephrectomy and living donor renal transplantation are successful for polycystic kidney disease: the University of Maryland experience. J Urol. 2009; 181:724–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasonography of polycystic kidney
- A Case of Renal Cell Carcinoma in Autosomal Dominant Polycystic Kidney Disease Hemodialyzed
- Severe and persistent hypotension after simultaneous nephrectomy and kidney transplantation in patients with chronic renal failure caused by polycystic kidney disease: Two cases report
- Autosomal Dominant Polycystic Kidney Disease Complicated by Aldosterone-producing Adrenal Adenoma
- A Case of Infantile Polycystic Kidney
