Two Microcatheter Technique for Embolization of Arteriovenous Fistula with Liquid Embolic Agent
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan, College of Medicine, Asan Medical Center, Seoul, Korea. dcsuh@amc.seoul.kr
- 2Department of Radiology, First Affiliated Hospital of Nanjing Medical University, Nanjing, China.
- KMID: 1910772
- DOI: http://doi.org/10.5469/neuroint.2014.9.1.32
Abstract
- Problem with embolization of arteriovenous fistula (AVF) with liquid embolic agent is its over-penetration into the veins or regurgitation to the proximal feeder without reaching the shunt point. We present a technique that controls the flow of AVF during embolization. Two microcatheter technique consists of positioning one microcatheter close to the AVF for embolization, and with another microcatheter at the proximal feeding artery to control the AVF flow by coiling. Selective angiograms obtained using a distally positioned microcatheter before and after coiling, were compared how much stagnant effect was achieved. Using two microcatheter technique, AVF occlusion was achieved with good penetration of glue to the venous side of the AVF. Its advantage is the ability to push glue into the shunt without causing over-penetration of glue or its reflux along the feeder. Two microcatheter technique was safe and effective in glue embolization of AVF and also expected to be applied with other liquid embolic agent like Onyx.
Figure
-
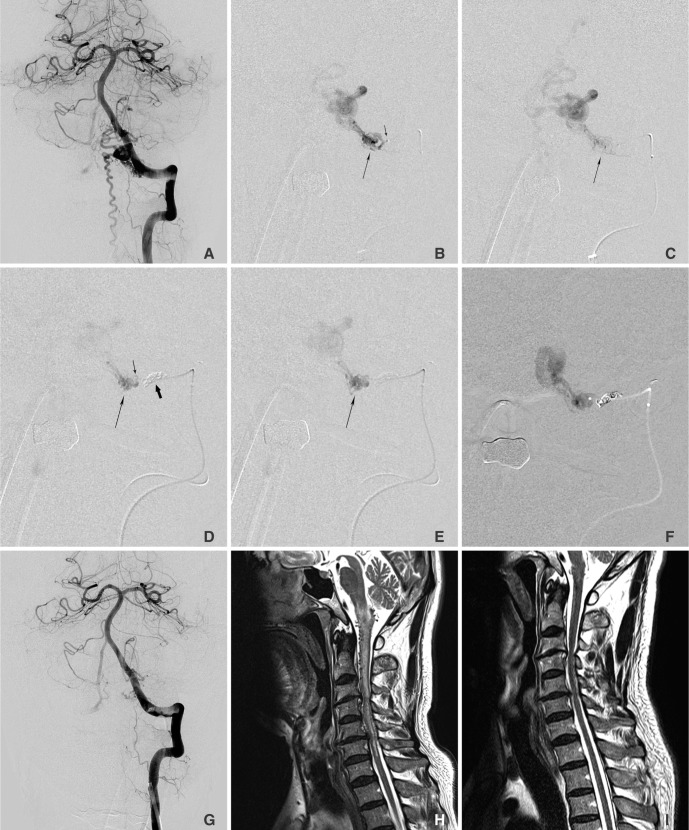
Fig. 1 A 53-year-old man presented with pain and sensory changes in the neck, both shoulders, and the upper extremities. A. Left vertebral angiogram shows a dural arteriovenous AVF at the C1 level. Note the perimedullary venous drainage. B & C. Selective angiogram obtained within a microcatheter (short, thin arrow in B) shows a AVF which reveals rapid washout of contrast agent due to the arterial inflow (long thin arrows in B & C). D & E. Same selective angiogram obtained after coiling (thick arrow in E) of the proximal feeder shows stagnant flow in the AVF (long, thin arrows in D & E). F. Note that the glue cast exactly fills the AVF and the adjacent vein. G. Left vertebral angiogram obtained after glue embolization showed no residual AVF. H & I. Comparison of the initial and the follow-up MRIs obtained three months later, shows complete disappearance of the intramedullary hyperintense edema caused by congestive venous myelopathy of the cervical spinal cord, as shown on T2WI with improvement of his symptoms.
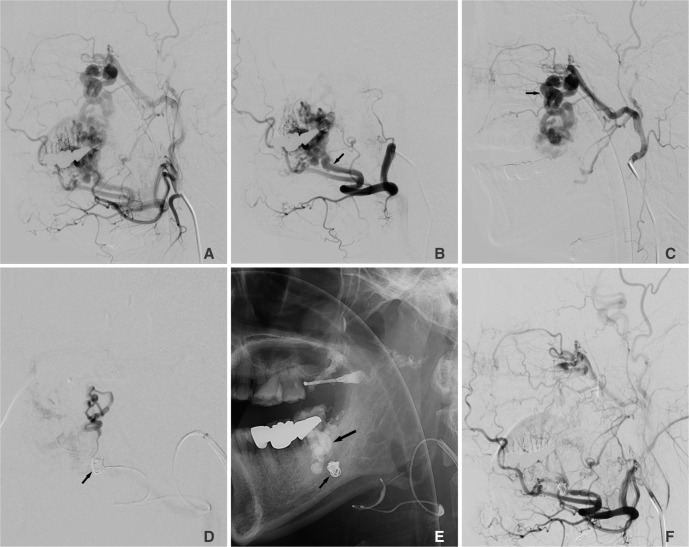
Fig. 2 A 42-year-old male presented with repeated ulcerative oral mucosal bleeding for 5 years. A. Left external carotid arteriogram shows an arteriovenous malformation in left cheek area. B. Left facial arteriogram shows an entangled vascular mass supplied by jugal branch (arrow) of the facial artery which is also supplied by branches (arrow) of the internal maxillary artery in figure C. Note dilated and tortuous feeders which preclude a microcatheter to reach the nidus. D. Distal microcatheter angiogram was obtained after proximal coiling (arrow) by proximal microcatheter after intra-arterial gelfoam and direct puncture glue embolizations in the lesion supplied by the internal maxillary artery. E. Note penetrated glue (a large arrow) beyond the protective coils (a small arrow). F. Final angiogram revealed no residual shunt and feeders. His oral ulcerative bleeding and mass effect in the cheek has improved so that further surgical resection was not required. There was no recurrence of ulceration or bleeding on 12 months follow-up period.

Fig. 3 Concept diagram of the two catheter technique. A. Two microcatheters are introduced into the site of the AVF feeder. AVF flow is controlled by coiling via the proximal catheter. B. Stable embolization is done by liquid embolic agent via the distal microcatheter. C. At the end of embolization, the distal microcatheter is removed under the support of the proximal catheter with undetached coil. D. The proximal microcatheter is removed after detachment of coil. E & F. Direct injection of liquid embolic agent with low concentration leads to migration of embolic agent into the vein without effective occlusion of AVF or regurgitation of embolic cast to the proximal feeder without effective penetration of the AVF.
Cited by 3 articles
-
Coil-Protected Technique for Liquid Embolization in Neurovascular Malformations
Keun Young Park, Jin Woo Kim, Byung Moon Kim, Dong Joon Kim, Joonho Chung, Chang Ki Jang, Jun-Hwee Kim
Korean J Radiol. 2019;20(8):1285-1292. doi: 10.3348/kjr.2019.0127.Embolization Tactics of Spinal Epidural Arteriovenous Fistulas
Abdulrahman Hamad Al-Abdulwahhab, Yunsun Song, Boseong Kwon, Dae Chul Suh
Neurointervention. 2021;16(3):252-259. doi: 10.5469/neuroint.2021.00220.Intrasaccular Flow Disruptor (Woven EndoBridge) Assisted Embolization of Vertebral Arteriovenous Fistulas
Oktay Algin
Neurointervention. 2024;19(1):61-64. doi: 10.5469/neuroint.2023.00514.
Reference
-
1. Kim DJ, Willinsky RA, Krings T, Agid R, Terbrugge K. Intracranial dural arteriovenous shunts: transarterial glue embolization--experience in 115 consecutive patients. Radiology. 2011; 258:554–561. PMID: 21177391.
Article2. Li MH, Tan HQ, Fang C, Zhu YQ, Wang W, Wang J, et al. Transarterial embolisation therapy of dural carotid-cavernous AVFe using low concentration n-butyl-cyanoacrylate. Acta Neurochir (Wien). 2008; 150:1149–1156. PMID: 18958391.3. Liu HM, Huang YC, Wang YH, Tu YK. Transarterial embolisation of complex cavernous sinus dural arteriovenous AVFe with low-concentration cyanoacrylate. Neuroradiology. 2000; 42:766–770. PMID: 11110083.4. Suh DC, Kim JH, Lee MS, Park S, Kim ST, Choi CG, et al. Penetration Difference of n-Butyl2-Cyanoacrylate into the Nidus in the Embolisation of Brain Arteriovenous Malformation. Interv Neuroradiol. 1998; 4:63–74. PMID: 20673392.5. Choi BS, Park JW, Kim JL, Kim SY, Park YS, Kwon HJ, et al. Treatment Strategy Based on Multimodal Management Outcome of Cavernous Sinus Dural Arteriovenous AVF (CSDAVF). Neurointervention. 2011; 6:6–12. PMID: 22125741.6. Rodesch G, Hurth M, Alvarez H, Tadie M, Lasjaunias P. Spinal cord intradural arteriovenous AVFe: anatomic, clinical, and therapeutic considerations in a series of 32 consecutive patients seen between 1981 and 2000 with emphasis on endovascular therapy. Neurosurgery. 2005; 57:973–983. PMID: 16284566.7. Jagadeesan BD, Grigoryan M, Hassan AE, Grande AW, Tummala RP. Endovascular Balloon-Assisted Embolization of Intracranial and Cervical Arteriovenous Malformations Using Dual Lumen Co-axial Balloon Microcatheters and Onyx: Initial Experience. Neurosurgery. 2013; 2. 25. [Epub ahead of print].8. Cohen JE, Moscovici S, Itshayek E. The advantages of balloon assistance in endovascular embolization of spinal dural arteriovenous AVFs. J Clin Neurosci. 2013; 20:141–143. PMID: 23146212.9. Shi ZS, Loh Y, Gonzalez N, Tateshima S, Feng L, Jahan R, et al. Flow control techniques for Onyx embolization of intracranial dural arteriovenous AVFe. J Neurointerv Surg. 2012; 5:311–316. PMID: 22591733.10. Andreou A, Ioannidis I, Nasis N. Transarterial balloon-assisted glue embolization of high-flow arteriovenous AVFs. Neuroradiology. 2008; 50:267–272. PMID: 17960371.11. Luo CB, Teng MM, Chang FC, Chang CY. Endovascular treatment of intracranial high-flow arteriovenous AVFs by Guglielmi detachable coils. J Chin Med Assoc. 2006; 69:80–85. PMID: 16570575.12. Nesbit GM, Barnwell SL. The use of electrolytically detachable coils in treating high-flow arteriovenous AVFs. AJNR Am J Neuroradiol. 1998; 19:1565–1569. PMID: 9763395.13. Lee C-S, Pyun HW, Chae EY, Kim K-K, Rhim SC, Suh DC. Reversible Aggravation of Neurological Deficits after Steroid Medication in Patients with Venous Congestive Myelopathy Caused by Spinal Arteriovenous Malformation. Interventional Neuroradiology. 2009; 15:325–329. PMID: 20465916.
Article14. Krings T, Lasjaunias PL, Hans FJ, Mull M, Nijenhuis RJ, Alvarez H, et al. Imaging in spinal vascular disease. Neuroimaging Clin N Am. 2007; 17:57–72. PMID: 17493539.
Article15. Suh DC, Kim HS, Baek HJ, Park JW, Kim KK, Rhim SC. Angioarchitecture of Spinal Dural Arteriovenous AVF - Evaluation with 3D Rotational Angiography. Neurointervention. 2012; 7:10–16. PMID: 22454779.16. Suh DC, Kim KS, Lim SM, Shi HB, Choi CG, Lee HK, et al. Technical feasibility of embolizing aneurysms with glue (N-butyl 2-cyanoacrylate): experimental study in rabbits. AJNR Am J Neuroradiol. 2003; 24:1532–1539. PMID: 13679265.17. Suh DC, Choi CG, Sung KB, Kim KK, Rhim SC. Spinal osseous epidural arteriovenous AVF with multiple small arterial feeders converging to a round AVFr nidus as a target of venous approach. AJNR Am J Neuroradiol. 2004; 25:69–73. PMID: 14729531.18. Nelson PK, Russell SM, Woo HH, Alastra AJ, Vidovich DV. Use of a wedged microcatheter for curative transarterial embolization of complex intracranial dural arteriovenous AVFs: indications, endovascular technique, and outcome in 21 patients. J Neurosurg. 2003; 98:498–506. PMID: 12650420.19. Shi HB, Suh DC, Lee HK, Lim SM, Kim DH, Choi CG, et al. Preoperative transarterial embolization of spinal tumor: embolization techniques and results. AJNR Am J Neuroradiol. 1999; 20:2009–2015. PMID: 10588136.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Snowballing Technique for High Flow Arteriovenous Fistula: A Technical Note
- Dural Arteriovenous Fistula Involving Transverse Sinus: Successful Embolization Using Onyx(R)
- Coil-Protected Technique for Liquid Embolization in Neurovascular Malformations
- Selective Arterial Embolization of Renal Arteriovenous Fistula and Arterial Aneurysm
- Iatrogenic Femoral Arteriovenous Fistulas: Endovascular Treatment with Coil Embolization in Two Patients
