Surgical Treatment for Lumbar Spinal Stenosis with Fracture in Multiple Osteoporotic Compression Fractures
- Affiliations
-
- 1Department of Orthopaedic Surgery, St. Vincent's Hospital, The Catholic University of Korea. hskoh@unitel.co.kr
- KMID: 1897025
- DOI: http://doi.org/10.4184/jkss.2005.12.1.75
Abstract
- STUDY DESIGN: A retrospective study.
OBJECTIVE
To analyze the outcome of the surgical treatment for lumbar spinal stenosis with fracture in multiple osteoporotic vertebral body compression fractures. SUMMARY OF LITERATURE REVIEW: An osteoporotic vertebral compression fracture, without neurological symptom, has mainly been treated with conservative care. Sometimes, vertebroplasty or kyphoplasty has been used as a surgical treatment. In the case of a single thoracolumbar fracture with neurological symptoms, not improved by conservative care, decompression, fusion and instrumentation through an anterior or a posterior approach has been attempted.
MATERIALS AND METHODS
10 patients, who had received surgical treatment for symptomatic lumbar spinal stenosis with fracture out of those with multiple osteoporotic vertebral body compression fractures, and over the age of 60, were assessed. The surgical treatment was performed on the patient with all of the following five criteria; (1) severe back pain caused by fractures, (2) neurological symptoms of lumbar spinal stenosis, (3) radiological evidences of stenosis by lumbar fracture, (4) no response to conservative treatment for over 3 months, and (5) adequate physical ability for daily living without a severe medical condition. The surgical procedure included: decompressive laminectomy, posterior instrumentation using pedicle screw fixation, and fusion in situ. The pedicle screws were located 2-3 above and below the most cephalad and caudad fractured vertebral bodies.
RESULTS
Clinically, favorable results were obtained in 8 of the 10 patients. In the roentgenographic assessment, the operated states were well maintained, without the metallic failure or instability. Halos around the pedicle screws were seen in 4 patients, but there was no significant evidence of loosening. There were no serious medical and systemic complications in the peri- and postoperative periods. Additional vertebral body fractures and pain were seen in 5 patients, but they had been well managed, conservatively.
CONCLUSION
Favorable clinical results could be expected for the surgical treatment of lumbar spinal stenosis, with fracture, in the patients with multiple osteoporotic vertebral fractures, as long as the surgical treatment was indicated exactly and carefully.
Keyword
MeSH Terms
Figure
-

Fig. 1. The plain roentgenography of 73-year old female patient. The AP (A) and lateral (B) films show type 2, biconcave fracture of L2 vertebral body and slight height loss of L3 vertebral body.
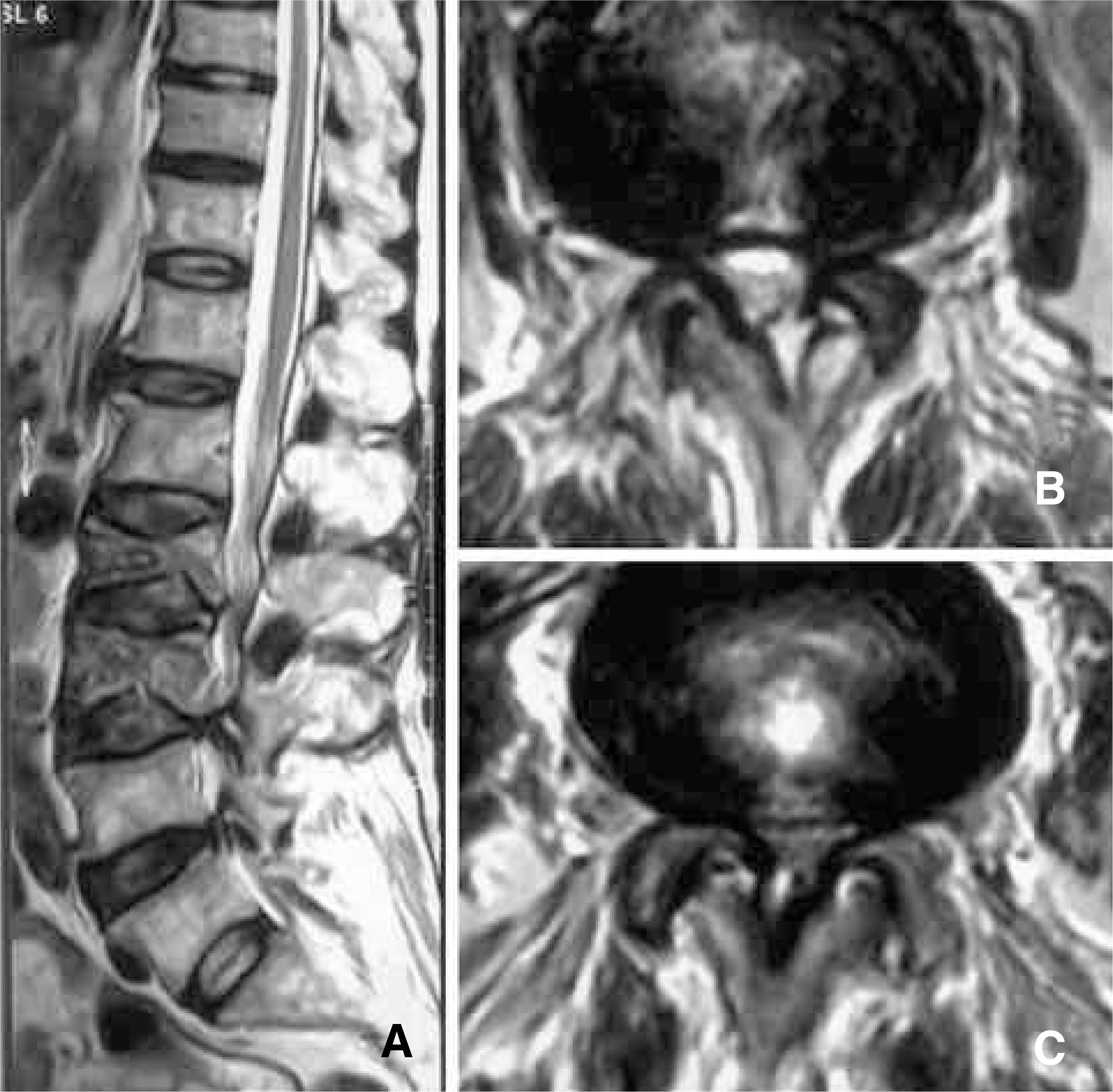
Fig. 2. The sagittal T2-weighted MRI (A) shows biconcave fractures at L2 and L3 vertebrae. The spinal canal is narrowed at L2-3, L3-4, and L4.5 interlaminar spaces. The axial T2-weighted MRI of L2-3 (B) and L3-4 (C) show central and lateral recess stenosis.
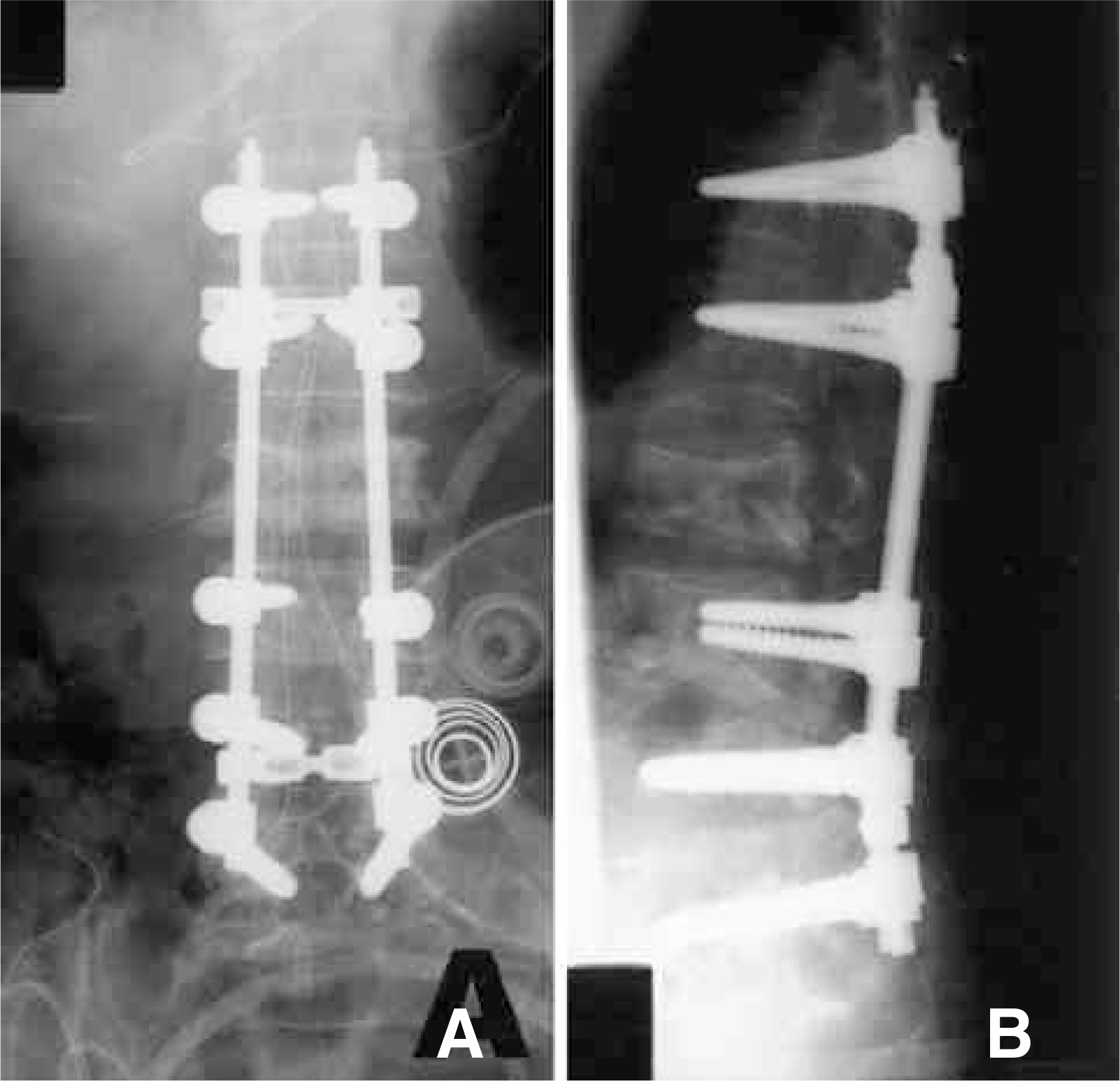
Fig. 3. The operation is done with L2-5 decompressive total laminectomy, posterior instrumentation, and fusion. There was no complication during peri- and postoperative period. She started ambulation with TLSO brace since 1 week after surgery. A) is AP and B) is lateral roentgenographic film.
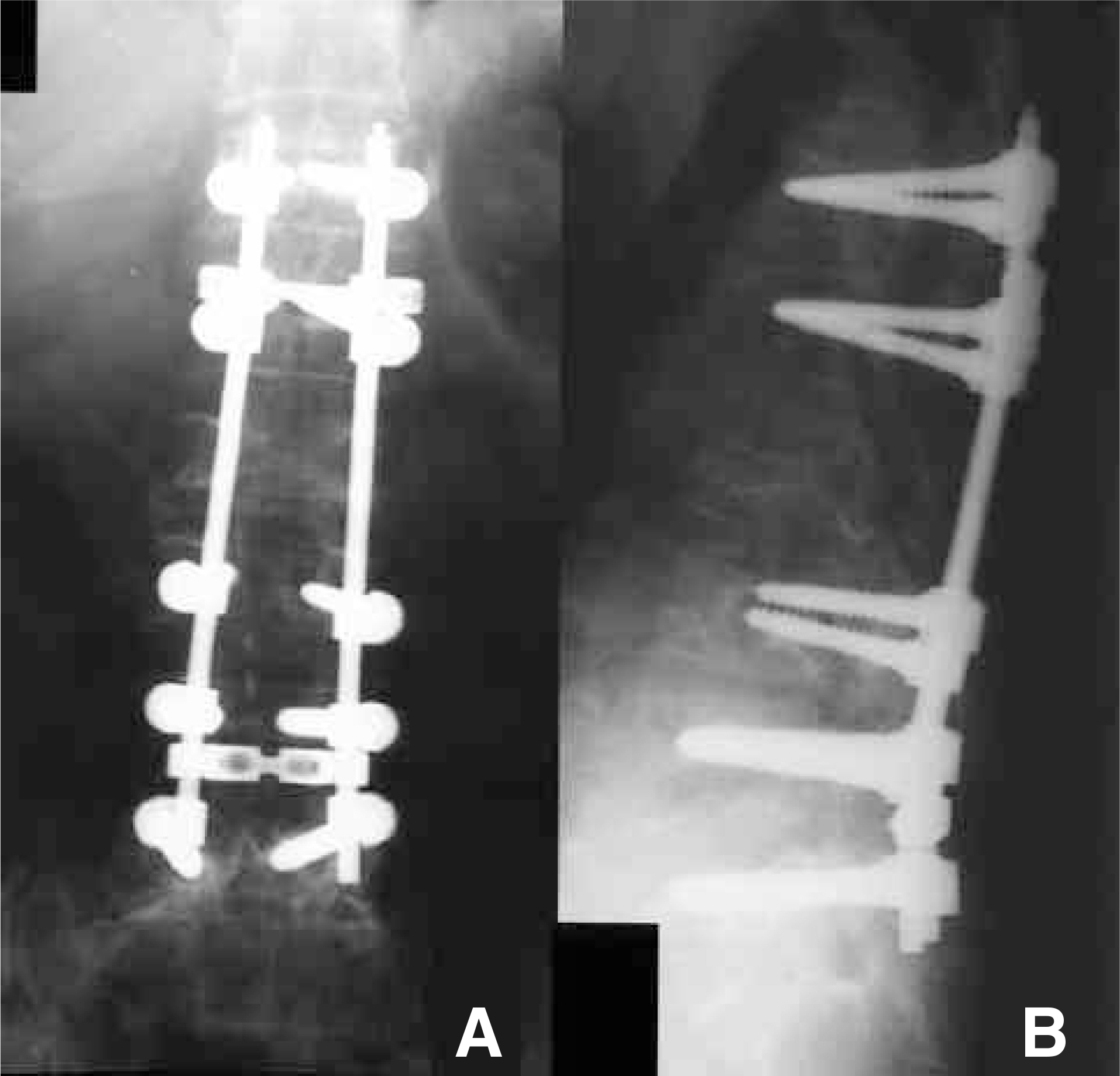
Fig. 4. At 30 months postoperatively, the operated site is maintained well. It is not easy to define the degree of bony fusion. But, there are no definite evidence of nonunion or implant failure. The clinical outcome of this patient is good and she just takes the medication for osteoporosis. A) is AP and B) is lateral roentgenographic film.
Reference
-
1). Adam PH. Osteoporosis. Clin Rheum Dis. 1981; 7:557–593.2). Kim D, Wang J, Kim I. The effect of nerve-root injection on pain relief in the management of osteoporotic vertebral fractures. J Kor Orthop Assoc. 2002; 37:385–391.
Article3). Lee YL, Yip KMH. The osteoporotic spine. Clin Orthop. 1996; 323:91–97.
Article4). Barr JD, Barr MS, Lemley TJ, McCann RM. Percutaneous vertebroplasty for pain relief and spinal stabilization. Spine. 2000; 25:923–928.
Article5). Cortet B, Coten A, Boutry N, Fliopo R, Duquesnoy B, Chastanet P, Delcambre B. Percutaneous vertebroplasty in the treatment of osteoporotic vertebral compression fractures: An open prospective study. J Rheumatol. 1999; 26:2222–2228.6). Grados F, Depriester C, Cayrolle G, Deramond HH, Fardellone P. Longterm observations of vertebral osteoporotic fractures treated by percutaneous vertebroplasty. Rheumatology. 2000; 39:1410–1414.
Article7). Jensen ME, Evans AJ, Mathis JM, et al. Percutaneous polymethylmethacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: Technical aspects. Am J Neuroradiol. 1997; 18:1897–1904.8). Lane JM, Johnson CE, Khan SN, Girardi FP, Cam-misa Jr FP. Minimally invasive options for the treatment of osteoporotic vertebral compression fractures. Orthop Clin North.9). Tohmeh AG, Mathis JM, Fenton DC, Levine AM, Belkoff SM. Biomechanical efficacy of unipedicular versus bipedicular vertebroplasty for the management of osteoporotic compression fractures. Spine. 1999; 24:1772–1776. Am. 2002; 33:431–438.
Article10). Theodorou DJ, Theodorou SJ, Duncan TD, Garfin SR, Wong WH. Percutaneous balloon kyphoplasty for the correction of spinal deformity in painful vertebral body compression fractures. Clin Imaging. 2002; 26:1–5.
Article11). Ha K, Kim K, Park S, Paek D, Ha J. The surgical treatment of osteoporotic vertebral collapse caused by minor trauma. J Kor Orthop Assoc. 1998; 33:105–216.
Article12). Heggeness MH. Spine fracture with neurological deficit in osteoporosis. Osteoporosis Int. 1993; 3:215–221.
Article13). Hu SS. Internal fixation in the osteoporotic spine. Spine. 1997; 22(suppl):S43–S48.
Article14). Kaneda KS, Ascano S, Hashimoto T, Satoh S, Fujiya M. The treatment of osteoporotic-posttraumatic vertebral collapse using the Kaneda-device and a bioactive ceramic vertebral prosthesis. Spine. 1992; 17(suppl):S295–S303.15). Kempinsky WH. Osteoporotic kyphosis with paraplegia. Neurology. 1986; 8:181–186.
Article16). Kim WJ, Kang JW, Yeom JS, Kim KH, Kim KJ, Lee SH, Choy WS. Surgical treatment of osteoporotic vertebral fracture with neurologic deficits in thoracolumbar junction Comparative analysis of the results according to the surgical method. J Kor Spine Surg. 2003; 10:321–326.17). Mochida J, Toh E, Chiba M, Nishimura K. Treatment of osteoporotic late collapse of a vertebral body of thoracic and lumbar spine. J Spinal Disord. 2001; 14:393–398.
Article18). Raiszadeh K, Akbarnia BA. Surgical management of adult kyphosis: idiopathic, posttraumatic, osteoporotic. Semin Spine Surg. 1998; 10:367–380.19). Shikata J, Yamamuro T, Ilda H, Shimizu K, Yoshikawa J. Surgical treatment for paraplegia resulting from vertebral fractures in senile osteoporosis. Spine. 1991; 15:1335–1341.
Article20). Kim E, Cho D, Kim J. A clinical analysis of long segment fusion with pedicle screw in degenerative lumbar spine. J Kor Spine Surg. 1999; 6:388–396.21). Roy-Camille R, Saillant G, Mazel C. Internal fixation of the lumbar spine with pedicle screw plating. Clin Orthop. 1986; 203:7–17.
Article22). Louis R. Fusion of the lumbar and sacral spine by internal fixation with screw plates. Clin Orthop. 1986; 203:18–33.
Article23). Devlin VJ, Boachie-Adjei O, Bradford DS, Ogilvie JW, Transfeldt EE. Treatment of adult spinal deformity with fusion to the sacrum using CD instrumentation. J Spinal Disord. 1991; 1:1–14.24). Chiba M, McLain RF, Yerby SA, Moseley TA, Smith TS, Benson DR. Short-segment pedicle screw fixation: Biomechanical analysis of supplemental hook fixation. Spine. 1996; 21:288–294.25). Halvorson TL, Kelly LA, Thomas KA, Whitecloud TS, Cook SD. Effects of bone mineral density on pedicle screw fixation. Spine. 1994; 19:2415–2420.
Article26). Hasegawa K, Takahashi HE, Uchiyama S, et al. An experimental study of a combination of method using a pedicle screw and laminar hook for the osteoporotic spine. Spine. 1997; 22:958–963.27). Soshi S, Shiba R, Kondo H, Murota K. An experimental study on transpedicular screw fixation in relation to osteoporosis in the lumbar spine. Spine. 1991; 16:1335–1341.28). Zindrick MR, Wiltse LL, Widell EH, et al. A biomechanical study of intrapedicular screw fixation in the lumbar spine. Clin Orthop. 1986; 203:99–112.29). Suzuki T, Abe E, Okuyama K, Sato K. Improving the pullout strength of pedicle screws by screw coupling. J Spinal Disord. 2001; 14:399–403.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Combined Treatment of Degenerative Spinal Stenosis and Osteoporotic Compression Fracture
- Vertebroplasty in the Multiple Osteoporotic Compression Fracture
- Osteoporotic Lumbar Compression Fracture in Patient with Ankylosing Spondylitis Treated with Kyphoplasty
- The Epidemiology and Importance of Osteoporotic Spinal Compression Fracture in South Korea
- Analysis of Osteoporotic Spinal Compression Fractures in Whole Spine Sagittal MR Images
