J Korean Soc Surg Hand.
2014 Dec;19(4):167-172. 10.12790/jkssh.2014.19.4.167.
Outcomes of the Sauve-Kapandji Procedure in Patients with Advanced Rheumatoid Arthritis
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul St. Mary's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea. ygchung@catholic.ac.kr
- KMID: 1896905
- DOI: http://doi.org/10.12790/jkssh.2014.19.4.167
Abstract
- PURPOSE
We evaluated the clinical and radiographic outcomes of the Sauve-Kapandji procedure for the treatment of advanced rheumatoid arthritis.
METHODS
Twenty-severn wrists in twenty-two patients were treated for advanced rheumatoid arthritis with Sauve-Kapandji procedure. Patients were evaluated in terms of wrist pain, bony union, instability of the ulnar proximal stump, ulnar stump pain, range of motion and other complications. Pain was evaluated using a visual analog scale. Radiographic evaluation included calculation of the carpal translation index to assess the extent of ulnar translation of the carpus.
RESULTS
The average visual analogue scale score improved from 4+/-1.85 preoperatively to 0.78+/-0.91 at the last follow-up (p=0.003). Bone unions in distal radioulnar joint were obtained in all 22 patients, 27 wrists at mean 10.74 weeks (range, 6-28 weeks) after operation. The supination/pronation range of motion was changed from 55/50 degrees preoperatively to 79/73 degrees at postoperative 6 months follow up (p=0.32). The mean carpal translation index did not change after the operation.
CONCLUSION
The Sauve-Kapandji procedure is a reliable methods of relieving pain, preserving range of motion (supination/pronation) and preventing ulnar translation of the carpus in managements of the severely destroyed distal radioulnar joints in rhematoid arthritis.
Keyword
MeSH Terms
Figure
-
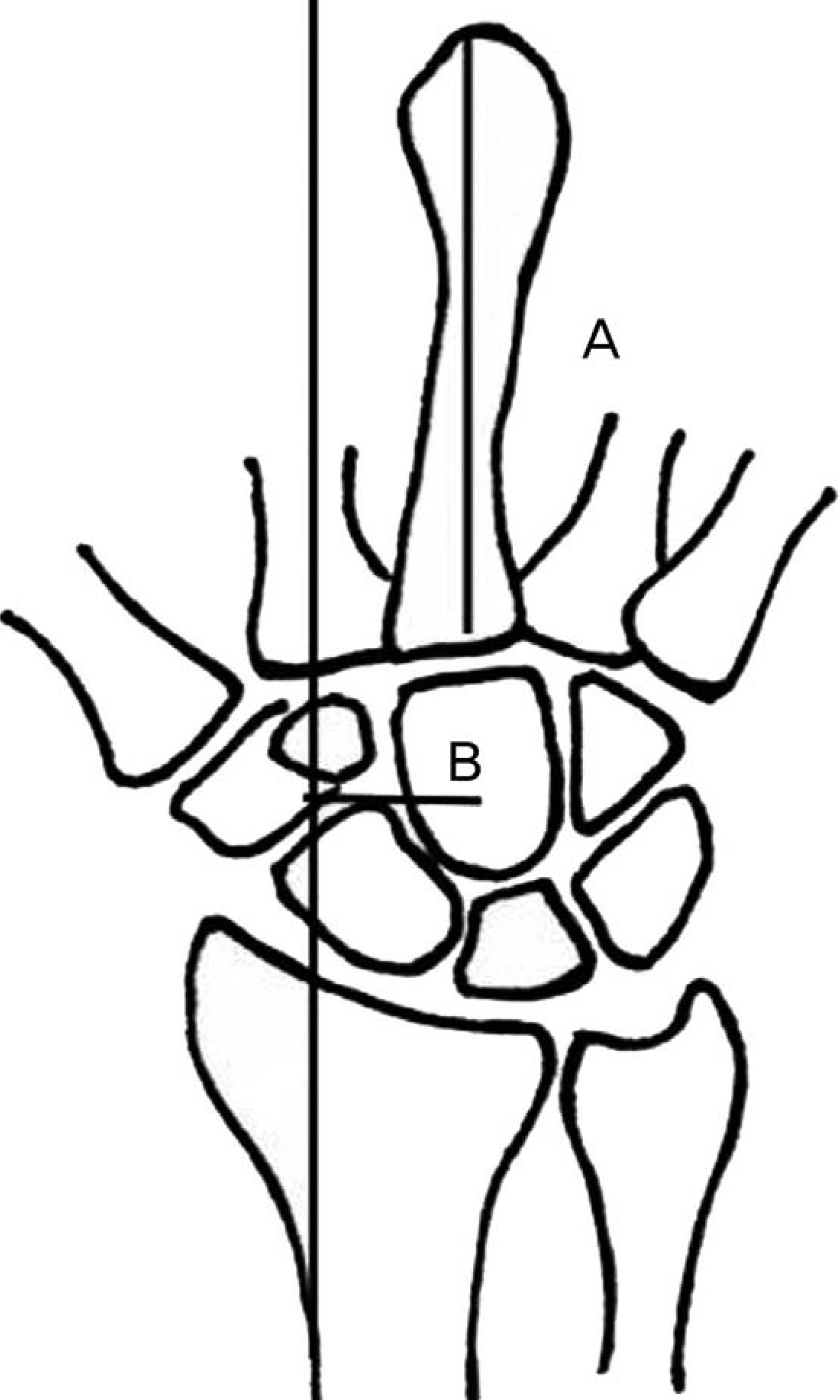
Fig. 1. The carpal translation index is calculated as the ratio of the distance between the center of the head of the capitate and a line drawn through the radial cortex of the radius B to the length of the third metacarpal A. This index normally measures 0.28±0.03 (mean and standard deviation).

Fig. 2. (A) Initial radiographs of right wrist of 40-year-old female patient showed rheumatoid arthritis. (B) Immediate postoperative radiographs. (C) Radiographs taken at postoperative 2 year showed complete osseus union.
Reference
-
1. Backdahl M. The caput ulnae syndrome in rheumatoid arthritis. A study of the morphology, abnormal anatomv and clinical picture. Acta Rheumatol Scand Suppl. 1963; 5:1–75.2. Couturier C, Alnot JY, Masmejean E. Dorsal instability of the ulnar stump following distal resection: hemi extensor-carpi-ulnaris stabilization procedure. Chir Main. 2002; 21:242–51.3. Fujita S, Masada K, Takeuchi E, Yasuda M, Komatsubara Y, Hashimoto H. Modified Sauve-Kapandji procedure for disorders of the distal radioulnar joint in patients with rheumatoid arthritis. J Bone Joint Surg Am. 2005; 87:134–9.4. Bell MJ, Hill RJ, McMurtry RY. Ulnar impingement syndrome. J Bone Joint Surg Br. 1985; 67:126–9.
Article5. Bieber EJ, Linscheid RL, Dobyns JH, Beckenbaugh RD. Failed distal ulna resections. J Hand Surg Am. 1988; 13:193–200.
Article6. Kessler I, Hecht O. Present application of the Darrach procedure. Clin Orthop Relat Res. 1970; 72:254–60.7. Minami A, Ogino T, Minami M. Treatment of distal radioulnar disorders. J Hand Surg Am. 1987; 12:189–96.
Article8. Newmeyer WL, Green DP. Rupture of digital extensor tendons following distal ulnar resection. J Bone Joint Surg Am. 1982; 64:178–82.
Article9. Bowers WH. Distal radioulnar joint arthroplasty: the hemiresection-interposition technique. J Hand Surg Am. 1985; 10:169–78.
Article10. Palmer AK, Werner FW. The triangular fibrocartilage complex of the wrist: anatomy and function. J Hand Surg Am. 1981; 6:153–62.11. Palmer AK, Werner FW. Biomechanics of the distal radioulnar joint. Clin Orthop Relat Res. 1984; 187:26–35.
Article12. Trumble T, Glisson RR, Seaber AV, Urbaniak JR. Forearm force transmission after surgical treatment of distal radioulnar joint disorders. J Hand Surg Am. 1987; 12:196–202.
Article13. Jensen CM. Synovectomy with resection of the distal ulna in rheumatoid arthritis of the wrist. Acta Orthop Scand. 1983; 54:754–9.
Article14. Taleisnik J, Gelberman RH, Miller BW, Szabo RM. The extensor retinaculum of the wrist. J Hand Surg Am. 1984; 9:495–501.
Article15. Rothwell AG, O'Neill L, Cragg K. Sauve-Kapandji procedure for disorders of the distal radioulnar joint: a simplified technique. J Hand Surg Am. 1996; 21:771–7.16. Lamey DM, Fernandez DL. Results of the modified Sauve-Kapandji procedure in the treatment of chronic posttraumatic derangement of the distal radioulnar joint. J Bone Joint Surg Am. 1998; 80:1758–69.17. Chu PJ, Lee HM, Hung ST, Shih JT. Stabilization of the proximal ulnar stump after the Darrach or Sauve-Kapandji procedure by using the extensor carpi ulnaris tendon. Hand (N Y). 2008; 3:346–51.18. Kapandji IA. The Kapandji-Sauve operation. Its techniques and indications in non rheumatoid diseases. Ann Chir Main. 1986; 5:181–93.19. Daecke W, Martini AK, Schneider S, Streich NA. Amount of ulnar resection is a predictive factor for ulnar instability problems after the Sauve-Kapandji procedure: a retrospective study of 44 patients followed for 1-13 years. Acta Orthop. 2006; 77:290–7.20. Wada T, Ogino T, Ishii S. Closed rupture of a finger extensor following the Sauve-Kapandji procedure: a case report. J Hand Surg Am. 1997; 22:705–7.21. Nakamura R, Tsunoda K, Watanabe K, Horii E, Miura T. The Sauve-Kapandji procedure for chronic dislocation of the distal radio-ulnar joint with destruction of the articular surface. J Hand Surg Br. 1992; 17:127–32.
