A Simple Method for Reconstruction of the Temporalis Muscle Using Contourable Strut Plate after Pterional Craniotomy: Introduction of the Surgical Techniques and Analysis of Its Efficacy
- Affiliations
-
- 1Department of Neurosurgery, Daegu Fatima Hospital, Daegu, Korea. paulyoonsoolee@hanmail.net
- KMID: 1879340
- DOI: http://doi.org/10.7461/jcen.2015.17.2.93
Abstract
OBJECTIVE
Pterional craniotomy (PC) using myocutaneous (MC) flap is a simple and efficient technique; however, due to subsequent inferior displacement (ID) of the temporalis muscle, it can cause postoperative deformities of the muscle such as depression along the inferior margin of the temporal line of the frontal bone (DTL) and muscular protrusion at the inferior portion of the temporal fossa (PITF). Herein, we introduce a simple method for reconstruction of the temporalis muscle using a contourable strut plate (CSP) and evaluate its efficacy.
MATERIALS AND METHODS
Patients at follow-ups between January 2014 and October 2014 after PCs were enrolled in this study. Their postoperative deformities of the temporalis muscle including ID, DTL, and PITF were evaluated. These PC cases using MC flap were classified according to two groups; one with conventional technique without CSP (MC Only) and another with reconstruction of the temporalis muscle using CSP (MC + CSP). Statistical analyses were performed for comparison between the two groups.
RESULTS
Lower incidences of ID of the muscle (p < 0.001), DTL (p < 0.001), and PITF (p = 0.001) were observed in the MC + CSP than in the MC Only group. The incidence of acceptable outcome was markedly higher in the MC + CSP group (p < 0.001). ID was regarded as a causative factor for DTL and PITF (p < 0.001 in both).
CONCLUSION
Reconstruction of the temporalis muscle using CSP after MC flap is a simple and efficient technique, which provides an outstanding outcome in terms of anatomical restoration of the temporalis muscle.
Keyword
MeSH Terms
Figure
-
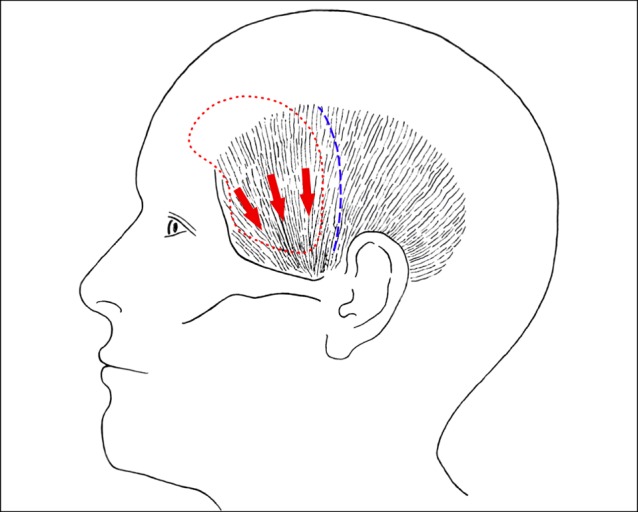
Fig. 1 The illustration depicts the course of fibers of the temporalis muscle and the direction of displacement, or sliding, (red arrows) of unattached temporalis muscle after pterional craniotomy (PC). The size and shape of PC (red dotted line) and the incision line on the temporalis muscle (blue dotted line) are also shown.
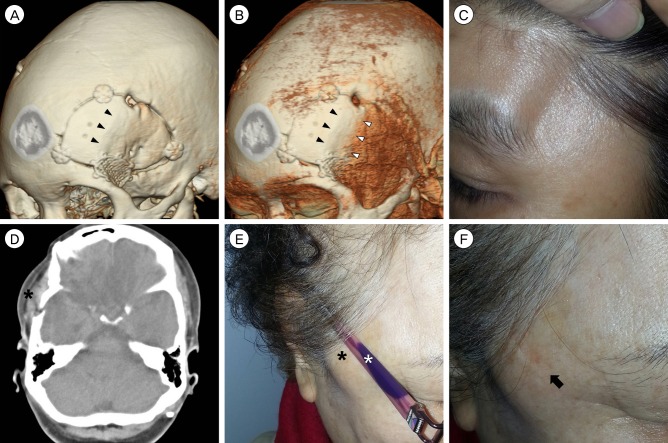
Fig. 2 Three-dimensional computed tomography (CT) scans (A, B) of a patient demonstrate the temporal line of the frontal bone (black arrowheads) and the displaced attachment site of the temporalis muscle (white arrowheads). A photograph (C) of the same patient shows a marked depression along the inferior margin of the temporal line of the frontal bone. The axial CT image (D) of a patient demonstrates a muscular protrusion at the inferior portion of the temporal fossa (black asterisk). Photographs (E, F) of the same patient show that this temporal protrusion (black asterisk) may cause discomfort when wearing glasses (white asterisk). Note the imprint on the skin (black arrow) after taking the glasses off.
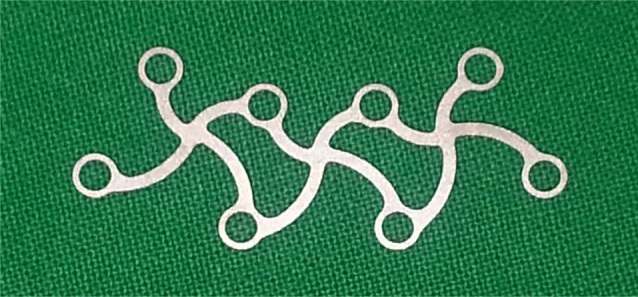
Fig. 3 The photograph shows the structure of a contourable strut plate (Synthes GmbH, Oberdorf, Switzerland). It is malleable and easily bent into various shapes which fit on the underlying bony contour.
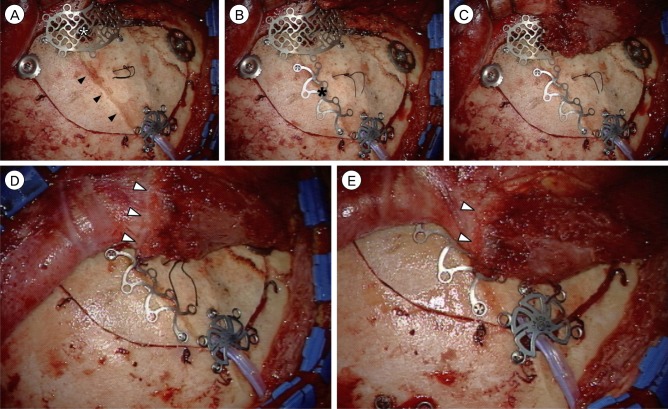
Fig. 4 Intraoperative photographs demonstrate the technique for reconstruction of the temporalis muscle using a contourable strut plate (CSP). (A) After fixation of the craniotomy bone using instruments such as mini-plates, titanium clamps, or burr hole covers, keyhole defect is repaired by temporal mesh floating technique (white asterisk). The temporal line of the frontal bone is indicated by black arrowheads. (B) A CSP (black asterisk) is slightly bent into the contour of the temporal line of the frontal bone and fixed to the temporal line using two low profile self-tapping screws. (C) The antero-inferior portion of the temporalis muscle is sutured over the temporal mesh. (D, E) The edge of the temporalis fascia and muscle (white arrowheads) is sutured and fixed to the CSP, which is the site of original attachment.
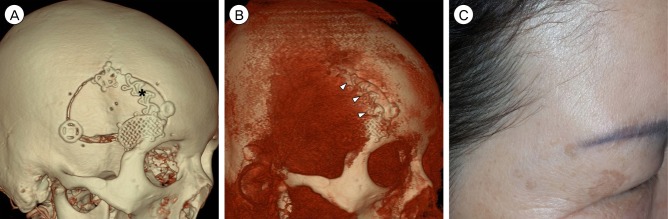
Fig. 5 Three-dimensional computed tomography (CT) scans (A, B) of a patient after reconstruction of the temporalis muscle using a contourable strut plate (CSP) (black asterisk) show anatomical restoration of the temporalis muscle at the temporal line (white arrowheads). A photograph (C) of the same patient shows an outstanding outcome without any deformities of the temporalis muscle.
Cited by 1 articles
-
Cosmetic outcome after electrocautery versus non-electrocautery dissection of the temporalis muscle for pterional craniotomy
Sang-Woo Lee, Yoon-Soo Lee, Min-Seok Lee, Sang-Jun Suh, Jeong-Ho Lee, Jin-Wook Kim
J Cerebrovasc Endovasc Neurosurg. 2022;24(1):16-23. doi: 10.7461/jcen.2021.E2021.07.001.
Reference
-
1. Ammirati M, Spallone A, Ma J, Cheatham M, Becker D. An anatomicosurgical study of the temporal branch of the facial nerve. Neurosurgery. 1993; 12. 33(6):1038–1043. discussion 1044PMID: 8133989.
Article2. Blaisdell FW, Steele M, Allen RE. Management of acute lower extremity arterial ischemia due to embolism and thrombosis. Surgery. 1978; 12. 84(6):822–834. PMID: 715701.3. Bowles AP Jr. Reconstruction of the temporalis muscle for pterional and cranio-orbital craniotomies. Surg Neurol. 1999; 11. 52(5):524–529. PMID: 10595774.
Article4. Brunori A, DiBenedetto A, Chiappetta F. Transosseous reconstruction of temporalis muscle for pterional craniotomy: technical note. Minim Invasive Neurosurg. 1997; 3. 40(1):22–23. PMID: 9138304.
Article5. Coscarella E, Vishteh AG, Spetzler RF, Seoane E, Zabramski JM. Subfascial and submuscular methods of temporal muscle dissection and their relationship to the frontal branch of the facial nerve. Technical note. J Neurosurg. 2000; 5. 92(5):877–880. PMID: 10794306.6. de Andrade Júnior FC, de Andrade FC, de Araujo Filho CM, Carcagnolo Filho J. Dysfunction of the temporalis muscle after pterional craniotomy for intracranial aneurysms. Comparative, prospective and randomized study of one flap versus two flaps dieresis. Arq Neuropsiquiatr. 1998; 1. 56(2):200–205. PMID: 9698728.7. Im TS, Lee YS, Suh SJ, Lee JH, Ryu KY, Kang DG. The efficacy of titanium burr hole cover for reconstruction of skull defect after burr hole trephination of chronic subdural hematoma. Korean J Neurotrauma. 2014; 10. 10(2):76–81.
Article8. Kadri PA, Al-Mefty O. The anatomical basis for surgical preservation of temporal muscle. J Neurosurg. 2004; 3. 100(3):517–522. PMID: 15035289.
Article9. Kang HJ, Lee YS, Suh SJ, Lee JH, Ryu KY, Kang DG. Comparative analysis of the mini-pterional and supraorbital keyhole craniotomies for unruptured aneurysms with numeric measurements of their geometric configurations. J Cerebrovasc Endovasc Neurosurg. 2013; 3. 15(1):5–12. PMID: 23593599.
Article10. Lee MS, Lee YS, Lee JH, Ryu KY, Kang DG. The efficacy of temporal mesh plate floating technique for keyhole site depression after frontotemporal craniotomy. J Korean Neurotraumatol Soc. 2011; 10. 7(2):78–82.
Article11. Matsumoto K, Akagi K, Abekura M, Ohkawa M, Tasaki O, Tomishima T. Cosmetic and functional reconstruction achieved using a split myofascial bone flap for pterional craniotomy. Technical note. J Neurosurg. 2001; 4. 94(4):667–670. PMID: 11302673.12. Miyazawa T. Less invasive reconstruction of the temporalis muscle for pterional craniotomy: modified procedures. Surg Neurol. 1998; 10. 50(4):347–351. PMID: 9817458.
Article13. Oikawa S, Mizuno M, Muraoka S, Kobayashi S. Retrograde dissection of the temporalis muscle preventing muscle atrophy for pterional craniotomy. Technical note. J Neurosurg. 1996; 2. 84(2):297–299. PMID: 8592239.14. Rhoton AL Jr. Anatomy of saccular aneurysms. Surg Neurol. 1980; 7. 14(1):59–66. PMID: 7414487.15. Salas E, Ziyal IM, Bejjani GK, Sekhar LN. Anatomy of the frontotemporal branch of the facial nerve and indications for interfascial dissection. Neurosurgery. 1998; 9. 43(3):563–568. PMID: 9733311.
Article16. Spetzler RF, Lee KS. Reconstruction of the temporalis muscle for the pterional craniotomy. Technical note. J Neurosurg. 1990; 10. 73(4):636–637. PMID: 2398396.17. Yaşargil MG. Microneurosurgery. Vol.I. New York, NY: Thieme;1984. p. 217–220.18. Yaşargil MG, Reichman MV, Kubik S. Preservation of the frontotemporal branch of the facial nerve using the interfascial temporalis flap for pterional craniotomy. Technical article. J Neurosurg. 1987; 9. 67(3):463–466. PMID: 3612281.19. Zager EL, DelVecchio DA, Bartlett SP. Temporal muscle microfixation in pterional craniotomies. Technical note. J Neurosurg. 1993; 12. 79(6):946–947. PMID: 8018137.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Subfascial Osteoplastic Bone Flap in Pterional Approach: Technical Note
- The Usefulness of Subfascial Temporalis Dissection Method in Pterional Craniotomy
- The Efficacy of Temporal Mesh Plate Floating Technique for Keyhole Site Depression after Frontotemporal Craniotomy
- A Textiloma on the Pterion : A Rarely Occurred Craniotomy Complication
- Intubation Difficulty in Patient with Pseudoankylosis of Temporo-mandibular Joint after Pterional Craniotomy
