Thoracolumbar Epidural Pannus Causing Paraplegia in Rhematoid Arthritis
- Affiliations
-
- 1Department of Orthopaedic Surgery, Chosun University School of Medicine, Gwangju, Korea. wwwpibak@daum.net
- KMID: 1851959
- DOI: http://doi.org/10.4055/jkoa.2015.50.3.249
Abstract
- Rheumatoid pannus involvement of the cervical spine like the atlanto-axial instability is common, but rheumatoid pannus involvement of the thoracolumbar spine is very rare. A 70-year-old woman with a 20-year medication history of rheumatoid arthritis (RA) came to a hospital because of paraparesis without trauma. Radiologic examination showed that the mass in the posterior aspect of the spinal canal of T12 to L2 was compressing the spinal cord. She underwent mass removal and posterior decompression. Histologic findings revealed lymphocytes with chronic inflammation which was seen in histologic findings of RA. Therefore, we supposed that the mass was a rheumatoid pannus and that it had caused paraparesis. We report a good result of paraparesis caused by thoracolumbar epidural pannus by RA in a patient who was treated with pannus removal and posterior decompression.
Keyword
MeSH Terms
Figure
-

Figure 1 Plain radiographs examination of the thoracolumbar spine at admission.

Figure 2 Axial computed tomography scans of the thoracolumbar spine. Calcified mass-like lesion in the posterior aspect of the central spinal canal of T12 to L2 resulted in compression of the spinal cord (arrow).

Figure 3 Magnetic resonance image. Unenhanced rod-like hyposignal intensity mass in the posterior aspect of the thecal space of T12 to L1 resulted in compression of the spinal cord. (A-C) Sagittal images (circles). (D-F) Axial images (arrows).

Figure 4 Operative finding: Chalklike materials in the posterior aspect of the spinal cord of T12 to L2.
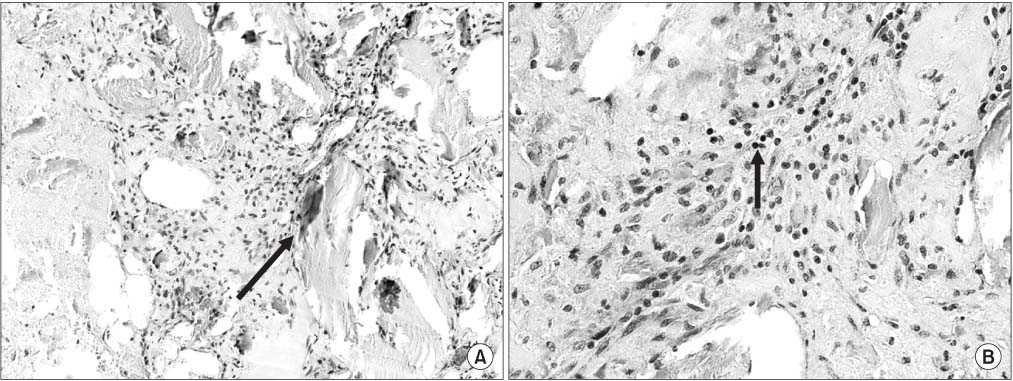
Figure 5 Histology finding of epidural mass. (A) In mid power field, eosinophilic bony chips (arrow) and stromal tissue with chronic inflammation are noted (H&E, ×200). (B) In high power field, stromal tissues with chronic inflammatory cells (lymphocytes) are noted (arrow) (H&E, ×400).
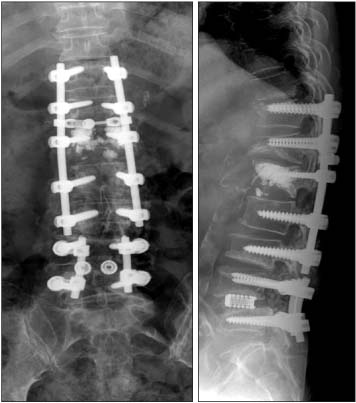
Figure 6 Plain radiographs one year after the operation.
Reference
-
1. Heywood AW, Meyers OL. Rheumatoid arthritis of the thoracic and lumbar spine. J Bone Joint Surg Br. 1986; 68:362–368.2. Taranto E, Leech M. Expression and function of cell cycle proteins in rheumatoid arthritis synovial tissue. Histol Histopathol. 2006; 21:205–211.3. Fujishiro M, Nozawa K, Kawasaki M, et al. Regenerating gene (REG) 1 alpha promotes pannus progression in patients with rheumatoid arthritis. Mod Rheumatol. 2012; 22:228–237.4. Kroft LJ, Reijnierse M, Kloppenburg M, Verbist BM, Bloem JL, van Buchem MA. Rheumatoid arthritis: epidural enhancement as an underestimated cause of subaxial cervical spinal stenosis. Radiology. 2004; 231:57–63.5. Shiratori K, Mennel HD, Bien S. Intraspinal pannus formation at C6 in a patient with rheumatoid arthritis causing severe cervical cord compression. A case report. Rheumatol Int. 2003; 23:192–194.6. Kinney WC, Scheetz RJ Jr, Strome M. Rheumatoid pannus of the cervical spine: a case report of an unusual cause of dysphagia. Ear Nose Throat J. 1999; 78:284.7. Catrina AI, Trollmo C, af Klint E, et al. Evidence that antitumor necrosis factor therapy with both etanercept and infliximab induces apoptosis in macrophages, but not lymphocytes, in rheumatoid arthritis joints: extended report. . Arthritis Rheum. 2005; 52:61–72.8. Rajak R, Wardle P, Rhys-Dillon C, Martin JC. Odontoid pannus formation in a patient with ankylosing spondylitis causing atlanto-axial instability. BMJ Case Rep. 2012; 2012:DOI: 10.1136/bcr.11.2011.5178.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Traumatic Spinal Epidural Hematoma in Ankylosing Spondylitis
- Infectious Spondylodiscitis Accompanied by Widespread Thoracolumbar Subdural Abscess
- Paraplegia following Epidural Analgesia
- Atlantoaxial Subluxation due to Psoriatic Arthritis
- Massive Epidural Hematoma Caused by Percutaneous Epidural Neuroplasty: A Case Report
