Improved Detection of Ischemic Heart Disease by Combining High-Frequency Electrocardiogram Analysis with Exercise Stress Echocardiography
- Affiliations
-
- 1Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. choijean5@gmail.com
- KMID: 1826558
- DOI: http://doi.org/10.4070/kcj.2013.43.10.674
Abstract
- BACKGROUND AND OBJECTIVES
Because the exercise treadmill test (ETT) based on ST-segment analysis is limited due to low sensitivity and specificity, there has been an interest in the additional analysis of high-frequency components of QRS (HFQRS) for the detection of coronary artery disease (CAD). We sought to evaluate the feasibility and clinical usefulness of HFQRS analysis during exercise stress echocardiography (ESE).
SUBJECTS AND METHODS
We evaluated 175 patients (age 57+/-9,118 men) who performed ESE and either coronary computed tomographic angiography or coronary angiography. ETT was performed using the HyperQ stress system for both conventional ST-segment analysis and HFQRS intensity analysis.
RESULTS
Thirty-two patients (31%) had significant CAD. The sensitivity and specificity of HFQRS analysis were 68.8% and 74.8%, respectively. The combined model, including HFQRS analysis and ESE, provided the best diagnostic accuracy, with the area under the receiver-operating characteristics curve (AUC) of 0.948 {95% confidence interval (CI)=0.913-0.984} compared with ST-segment analysis (AUC 0.679, 95% CI=0.592-0.766).
CONCLUSION
HFQRS analysis during ESE is feasible and may provide additional diagnostic information for the detection of significant CAD.
MeSH Terms
Figure
-
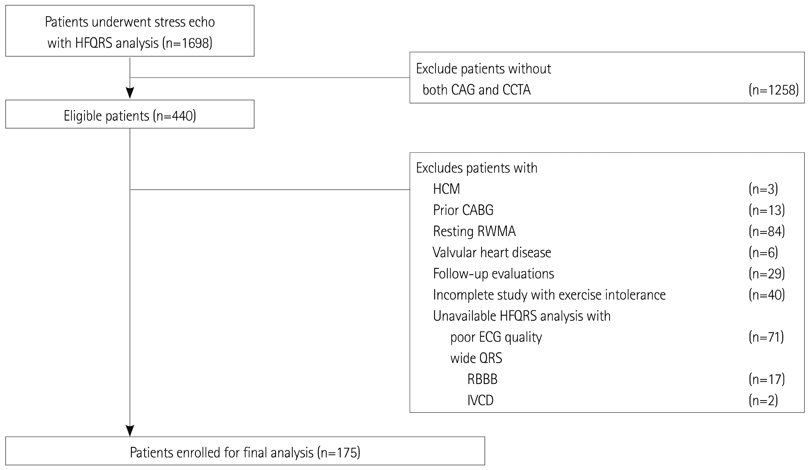
Fig. 1 Flowchart of enrollment of study patients. CAG: coronary angiography, CCTA: coronary computed tomographic angiography, HCM: hypertrophic cardiomyopathy, CABG: coronary artery bypass graft surgery, RWMA: regional wall motion abnormality, RBBB: right bundle branch block, IVCD: intraventricular conduction delay, ECG: electrocardiography, HFQRS: high-frequency components of QRS.
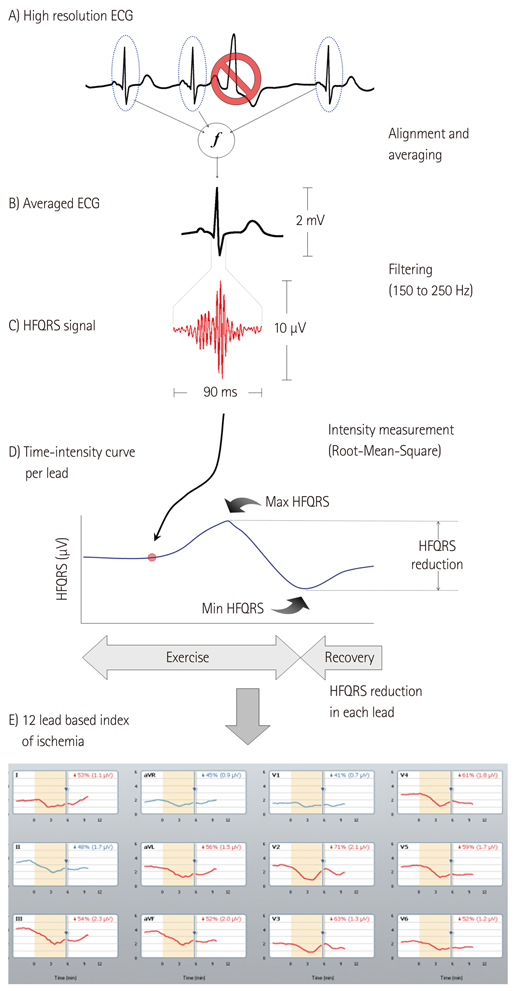
Fig. 2 Schematic flowchart of high-frequency QRS analysis and representative case. Modified from figures by Sharir et al.8) ECG: electrocardiography, HFQRS: high-frequency components of QRS.
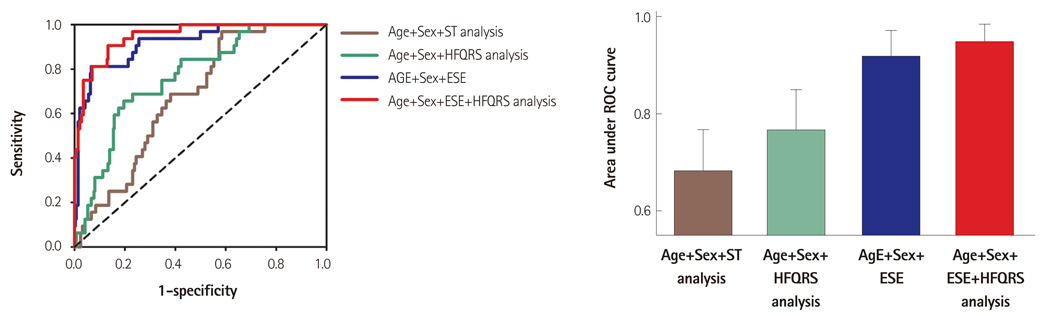
Fig. 3 Receiver operational characteristic (ROC) curves for the diagnosis of significant coronary artery disease. Note the incremental value of HFQRS and/or ESE over ST-segment analysis and clinical variables. HFQRS: high frequency QRS analysis, ESE: exercise stress echocardiography.
Reference
-
1. Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). Circulation. 2002; 106:1883–1892.2. Lucas FL, DeLorenzo MA, Siewers AE, Wennberg DE. Temporal trends in the utilization of diagnostic testing and treatments for cardiovascular disease in the United States, 1993-2001. Circulation. 2006; 113:374–379.3. Nedeljkovic I, Ostojic M, Beleslin B, et al. Comparison of exercise, dobutamine-atropine and dipyridamole-atropine stress echocardiography in detecting coronary artery disease. Cardiovasc Ultrasound. 2006; 4:22.4. Abboud S, Cohen RJ, Selwyn A, Ganz P, Sadeh D, Friedman PL. Detection of transient myocardial ischemia by computer analysis of standard and signal-averaged high-frequency electrocardiograms in patients undergoing percutaneous transluminal coronary angioplasty. Circulation. 1987; 76:585–596.5. Pettersson J, Pahlm O, Carro E, et al. Changes in high-frequency QRS components are more sensitive than ST-segment deviation for detecting acute coronary artery occlusion. J Am Coll Cardiol. 2000; 36:1827–1834.6. Schlegel TT, Kulecz WB, DePalma JL, et al. Real-time 12-lead high-frequency QRS electrocardiography for enhanced detection of myocardial ischemia and coronary artery disease. Mayo Clin Proc. 2004; 79:339–350.7. Toledo E, Lipton JA, Warren SG, et al. Detection of stress-induced myocardial ischemia from the depolarization phase of the cardiac cycle--a preliminary study. J Electrocardiol. 2009; 42:240–247.8. Sharir T, Merzon K, Kruchin I, et al. Use of electrocardiographic depolarization abnormalities for detection of stress-induced ischemia as defined by myocardial perfusion imaging. Am J Cardiol. 2012; 109:642–650.9. Gianrossi R, Detrano R, Mulvihill D, et al. Exercise-induced ST depression in the diagnosis of coronary artery disease. A meta-analysis. Circulation. 1989; 80:87–98.10. Higgins JP, Higgins JA. Electrocardiographic exercise stress testing: an update beyond the ST segment. Int J Cardiol. 2007; 116:285–299.11. Kligfield P, Lauer MS. Exercise electrocardiogram testing: beyond the ST segment. Circulation. 2006; 114:2070–2082.12. Okin PM, Kligfield P. Heart rate adjustment of ST segment depression and performance of the exercise electrocardiogram: a critical evaluation. J Am Coll Cardiol. 1995; 25:1726–1735.13. Abboud S, Berenfeld O, Sadeh D. Simulation of high-resolution QRS complex using a ventricular model with a fractal conduction system. Effects of ischemia on high-frequency QRS potentials. Circ Res. 1991; 68:1751–1760.14. Abboud S, Cohen RJ, Sadeh D. A spectral analysis of the high frequency QRS potentials observed during acute myocardial ischemia in dogs. Int J Cardiol. 1990; 26:285–290.15. Mor-Avi V, Shargorodsky B, Abboud S, Laniado S, Akselrod S. Effects of coronary occlusion on high-frequency content of the epicardial electrogram and body surface electrocardiogram. Circulation. 1987; 76:237–243.16. Abboud S. Subtle alterations in the high-frequency QRS potentials during myocardial ischemia in dogs. Comput Biomed Res. 1987; 20:384–395.17. Lauer M, Froelicher ES, Williams M, Kligfield P. American Heart Association Council on Clinical Cardiology, Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention. Exercise testing in asymptomatic adults: a statement for professionals from the American Heart Association Council on Clinical Cardiology, Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention. Circulation. 2005; 112:771–776.18. Froelicher VF, Lehmann KG, Thomas R, et al. The electrocardiographic exercise test in a population with reduced workup bias: diagnostic performance, computerized interpretation, and multivariable prediction Veterans Affairs Cooperative Study in Health Services #016 (QUEXTA) Study Group Quantitative Exercise Testing and Angiography. Ann Intern Med. 1998; 128(12 Pt 1):965–974.19. Geleijnse ML, Fioretti PM, Roelandt JR. Methodology, feasibility, safety and diagnostic accuracy of dobutamine stress echocardiography. J Am Coll Cardiol. 1997; 30:595–606.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of exercise stress echocardiography and 99Tc-MIBI heart SPECT for the detection of coronary artery disease
- A Study on the Electrocardiographic Diagnosis of Ischemic Heart Disease: 1. Positive Criteria for Postexercise Electrocardiogram
- The Usefulness of Exercise Stress Echocardiography in Diagnosis of Coronary Artery Disease
- Doppler Assessment of Mitral and Aortic flow in Exercise Stress Echocardiography
- Role of Echocardiography in the Management of Cardiac Disease in Women
