Diagnostic Usefulness of Dual-Energy Computed Tomography in Evaluation of the Severity of Acute Pulmonary Thromboembolism
- Affiliations
-
- 1Department of Radiology, Chonnam National University Hospital, Gwangju, Korea. yhkim001@jnu.ac.kr
- 2Department of Radiology, Chonnam National University Hwasun Hospital, Hwasun, Korea.
- 3Department of Radiology, Chonnam National University Medical School, Gwangju, Korea.
- 4Department of Radiology, Chonnam National University Bitgoeul Hospital, Gwangju, Korea.
- KMID: 1823933
- DOI: http://doi.org/10.3348/jksr.2015.72.1.38
Abstract
- PURPOSE
To evaluate the usefulness of dual-energy computed tomography (DECT) in severity assessment of patients with acute pulmonary thromboembolism (APTE).
MATERIALS AND METHODS
We evaluated 61 patients diagnosed as APTE from 2011 to 2012 in a retrospective analysis of the severity assessment indices according to Criteria by European Society of Cardiology as well as pulmonary CT angiographic obstruction score (OS) and lung perfusion index (pulmonary perfusion defect score; DS) by DECT. The correlation between OS, DS and the severity of pulmonary thromboembolism was evaluated using logit analysis.
RESULTS
Patients with high OS also showed significantly higher DS values (p < 0.001). There was a significant correlation between both the OS and DS values and the severity of the pulmonary thromboembolism using simple sequence logit analysis (p < 0.001). However, only the DS value showed a very high correlation with the severity of pulmonary thromboembolism using multiple sequence logit analysis.
CONCLUSION
DECT provides a more useful marker for the diagnosis and severity assessment of pulmonary thromboembolism by checking the degree of lung perfusion as well as determining the existence of APTE in patients with suspected pulmonary thromboembolism.
Figure
-
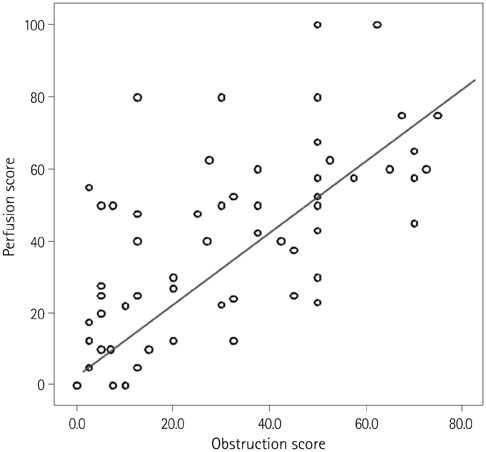
Fig. 1 Correlation between pulmonary perfusion defect score and pulmonary CT angiographic obstruction score in patient based analysis.
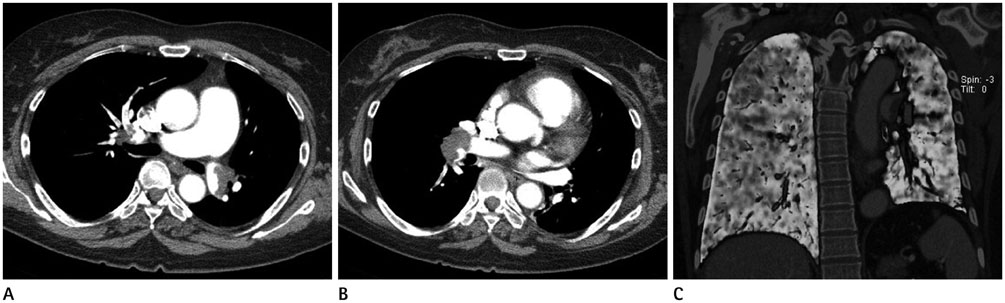
Fig. 2 57-year-old woman with pulmonary thromboembolism, who had high obstruction score (75/100) and low perfusion defect score (42.5/100). Pulmonary CT angiography (A, B) shows extensive thromboembolic filling defect in both main, lobar, and segmental pulmonary arteries, but lung perfusion is relatively well preserved on pulmonary perfusion image (C).
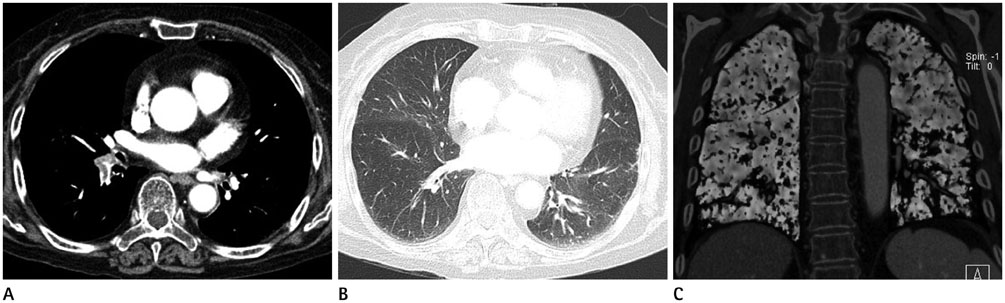
Fig. 3 82-year-old woman with pulmonary thromboembolism, who had low obstruction score (12.5/100) but relatively high perfusion defect score (60/100). Pulmonary CT angiography (A) shows only focal thromboembolic filling defect in right lower lobar and segmental pulmonary arteries, but prominent low attenuation on lung window setting image (B) and perfusion defect areas on pulmonary perfusion image (C).
Reference
-
1. Torbicki A, Perrier A, Konstantinides S, Agnelli G, Galiè N, Pruszczyk P, et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J. 2008; 29:2276–2315.2. Anderson FA Jr, Wheeler HB, Goldberg RJ, Hosmer DW, Patwardhan NA, Jovanovic B, et al. The Worcester DVT Study. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. Arch Intern Med. 1991; 151:933–938.3. Kasper W, Konstantinides S, Geibel A, Olschewski M, Heinrich F, Grosser KD, et al. Management strategies and determinants of outcome in acute major pulmonary embolism: results of a multicenter registry. J Am Coll Cardiol. 1997; 30:1165–1171.4. Wildberger JE, Schoepf UJ, Mahnken AH, Herzog P, Ditt H, Niethammer MU, et al. Approaches to CT perfusion imaging in pulmonary embolism. Semin Roentgenol. 2005; 40:64–73.5. Chung MJ, Goo JM, Im JG, Lee KS, Kim KG, Park JH. CT perfusion image of the lung: value in the detection of pulmonary embolism in a porcine model. Invest Radiol. 2004; 39:633–640.6. Hoey ET, Mirsadraee S, Pepke-Zaba J, Jenkins DP, Gopalan D, Screaton NJ. Dual-energy CT angiography for assessment of regional pulmonary perfusion in patients with chronic thromboembolic pulmonary hypertension: initial experience. AJR Am J Roentgenol. 2011; 196:524–532.7. Chae EJ, Seo JB, Jang YM, Krauss B, Lee CW, Lee HJ, et al. Dual-energy CT for assessment of the severity of acute pulmonary embolism: pulmonary perfusion defect score compared with CT angiographic obstruction score and right ventricular/left ventricular diameter ratio. AJR Am J Roentgenol. 2010; 194:604–610.8. Thieme SF, Johnson TR, Lee C, McWilliams J, Becker CR, Reiser MF, et al. Dual-energy CT for the assessment of contrast material distribution in the pulmonary parenchyma. AJR Am J Roentgenol. 2009; 193:144–149.9. Flohr TG, McCollough CH, Bruder H, Petersilka M, Gruber K, Süss C, et al. First performance evaluation of a dual-source CT (DSCT) system. Eur Radiol. 2006; 16:256–268.10. Johnson TR, Krauss B, Sedlmair M, Grasruck M, Bruder H, Morhard D, et al. Material differentiation by dual energy CT: initial experience. Eur Radiol. 2007; 17:1510–1517.11. Dogan H, Kroft LJ, Huisman MV, van der Geest R, Li OY, Lamb HJ, et al. Assessment of right ventricular function in acute pulmonary embolism using ECG-synchronized MDCT. AJR Am J Roentgenol. 2010; 195:909–915.12. Seon HJ, Kim KH, Lee WS, Choi S, Yoon HJ, Ahn Y, et al. Usefulness of computed tomographic pulmonary angiography in the risk stratification of acute pulmonary thromboembolism. Comparison with cardiac biomarkers. Circ J. 2011; 75:428–436.13. Qanadli SD, El Hajjam M, Vieillard-Baron A, Joseph T, Mesurolle B, Oliva VL, et al. New CT index to quantify arterial obstruction in pulmonary embolism: comparison with angiographic index and echocardiography. AJR Am J Roentgenol. 2001; 176:1415–1420.14. Petersson J, Sánchez-Crespo A, Larsson SA, Mure M. Physiological imaging of the lung: single-photon-emission computed tomography (SPECT). J Appl Physiol (1985). 2007; 102:468–476.15. Ryan KL, Fedullo PF, Davis GB, Vasquez TE, Moser KM. Perfusion scan findings understate the severity of angiographic and hemodynamic compromise in chronic thromboembolic pulmonary hypertension. Chest. 1988; 93:1180–1185.16. Kreitner KF, Kunz RP, Ley S, Oberholzer K, Neeb D, Gast KK, et al. Chronic thromboembolic pulmonary hypertension-assessment by magnetic resonance imaging. Eur Radiol. 2007; 17:11–21.17. Ley S, Kreitner KF, Fink C, Heussel CP, Borst MM, Kauczor HU. Assessment of pulmonary hypertension by CT and MR imaging. Eur Radiol. 2004; 14:359–368.18. Nikolaou K, Schoenberg SO, Attenberger U, Scheidler J, Dietrich O, Kuehn B, et al. Pulmonary arterial hypertension: diagnosis with fast perfusion MR imaging and high-spatial-resolution MR angiography--preliminary experience. Radiology. 2005; 236:694–703.19. Fink C, Thieme S, Ley S, Clevert D, Reiser MF, Kauczor HU, et al. [MRI of pulmonary embolism]. Radiologe. 2007; 47:708–715.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Advances in Multidetector CT Diagnosis of Pediatric Pulmonary Thromboembolism
- Effectiveness of Virtual Non-Enhanced Images Acquired by Dual-Energy Computed Tomography in Evaluation of Patients with Suspected Acute Appendicitis
- Dual-Layer Computed Tomography in Cardiovascular Imaging
- Dual-Energy CT for Pulmonary Embolism: Current and Evolving Clinical Applications
- Ultrasonography and dual-energy computed tomography: impact for the detection of gouty deposits
