Impaired Global Right Ventricular Longitudinal Strain Predicts Long-Term Adverse Outcomes in Patients with Pulmonary Arterial Hypertension
- Affiliations
-
- 1Department of Cardiovascular Medicine, The Cleveland Clinic Foundation, Cleveland, OH, USA. jthomas8@nmh.org
- 2Cardiology Division of Internal Medicine, Chungnam National University, Chungnam National University Hospital, Daejeon, Korea.
- 3Pulmonary and Critical Care Medicine, The Cleveland Clinic Foundation, Cleveland, OH, USA.
- 4Center for Heart Valve Disease, Bluhm Cardiovascular Institute, Northwestern Memorial Hospital, Chicago, IL, USA.
- KMID: 1806917
- DOI: http://doi.org/10.4250/jcu.2015.23.2.91
Abstract
- BACKGROUND
New 2-dimensional strain echocardiography enables quantification of right ventricular (RV) mechanics by assessing global longitudinal strain of RV (GLSRV) in patients with pulmonary arterial hypertension (PAH). However, the prognostic significance of impaired GLSRV is unclear in these patients.
METHODS
Comprehensive echocardiography was performed in 51 consecutive PAH patients without atrial fibrillation (40 females, 48 +/- 14 years old) with long-term follow-up. GLSRV was measured with off-line with velocity vector imaging (VVI, Siemens Medical System, Mountain View, CA, USA).
RESULTS
GLSRV showed significant correlation with RV fractional area change (r = -0.606, p < 0.001), tricuspid annular plane systolic excursion (r = -0.579, p < 0.001), and RV Tei index (r = 0.590, p < 0.001). It showed significant correlations with pulmonary vascular resistance (r = 0.469, p = 0.001) and B-natriuretic peptide concentration (r = 0.351, p = 0.012). During a clinical followup time (45 +/- 15 months), 20 patients experienced one or more adverse events (12 death, 2 lung transplantation, and 15 heart failure hospitalization). After multivariate analysis, age [hazard ratio (HR) = 2.343, p = 0.040] and GLSRV (HR = 2.122, p = 0.040) were associated with adverse clinical events. Age (HR = 3.200, p = 0.016) and GLSRV (HR = 2.090, p = 0.042) were also significant predictors of death. Impaired GLSRV (> or = -15.5%) was associated with lower event-free survival (HR = 4.906, p = 0.001) and increased mortality (HR = 8.842, p = 0.005).
CONCLUSION
GLSRV by VVI showed significant correlations with conventional echocardiographic parameters indicating RV systolic function. Lower GLSRV (> or = -15.5%) was significantly associated with presence of adverse clinical events and deaths in PAH patients.
MeSH Terms
Figure
-
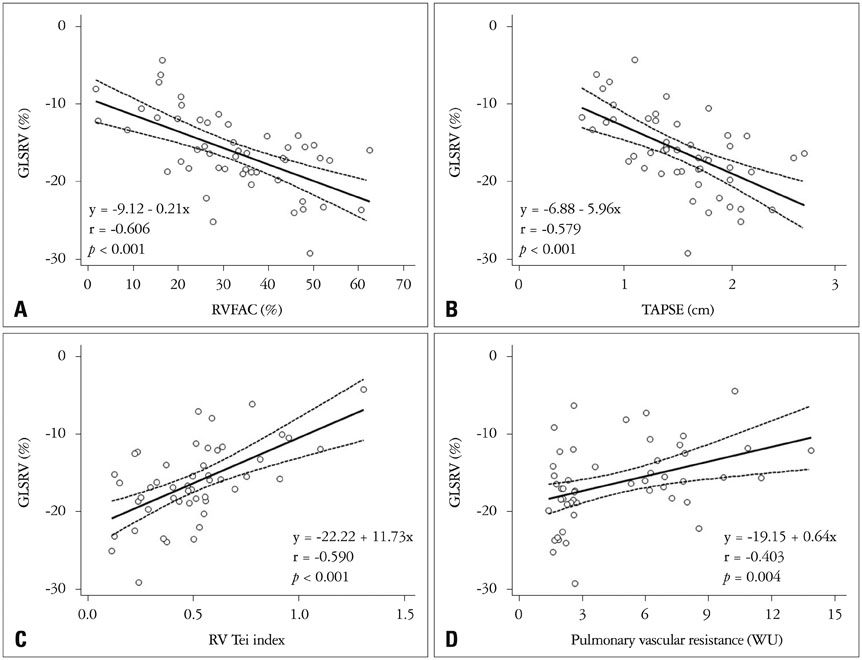
Fig. 1 Correlations between global longitudinal strain of right ventricle (GLSRV) and echocardiographic parameters. GLSRV shows good negative correlation with RV fractional area change (RVFAC, A), tricuspid annular plane systolic excursion (TAPSE, B), and RV Tei index (C). Also, GLSRV demonstrates significant correlation with pulmonary vascular resistance calculated by echocardiography (D).
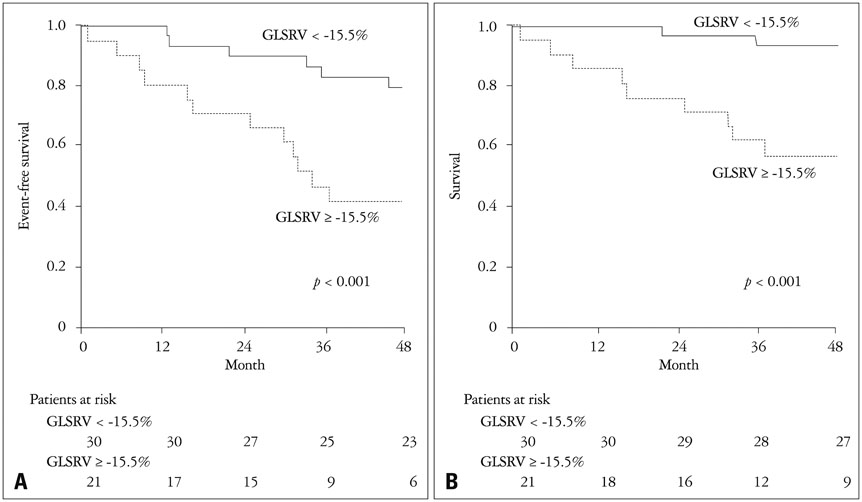
Fig. 2 Event-free survival and total survival curve by Kaplan-Meier analysis. Patients with impaired global longitudinal strain of right ventricle (GLSRV) (≥ -15.5%) showed lower event-free survival (80 ± 7% vs. 42 ± 11% at 4 years, p < 0.001) (A) and lower survival (93 ± 5% vs. 57 ± 11% at 4 years, p < 0.001) (B) than preserved GLSRV patients. p value refers to Log-rank test.
Reference
-
1. Bogaard HJ, Abe K, Vonk Noordegraaf A, Voelkel NF. The right ventricle under pressure: cellular and molecular mechanisms of right-heart failure in pulmonary hypertension. Chest. 2009; 135:794–804.2. Sitbon O, Humbert M, Nunes H, Parent F, Garcia G, Hervé P, Rainisio M, Simonneau G. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol. 2002; 40:780–788.3. Condliffe R, Kiely DG, Coghlan JG, Gibbs JS, Wort SJ, Corris PA, Peacock AJ, Pepke-Zaba J. Adult Pulmonary Hypertension Service of the United Kingdom. Survival in pulmonary hypertension registries: the importance of incident cases. Chest. 2011; 139:1547–1548. author reply 1548-9.4. D'Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991; 115:343–349.5. Sandoval J, Bauerle O, Palomar A, Gómez A, Martínez-Guerra ML, Beltrán M, Guerrero ML. Survival in primary pulmonary hypertension. Validation of a prognostic equation. Circulation. 1994; 89:1733–1744.6. Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010; 23:685–713. quiz 786-87. Giusca S, Dambrauskaite V, Scheurwegs C, D'hooge J, Claus P, Herbots L, Magro M, Rademakers F, Meyns B, Delcroix M, Voigt JU. Deformation imaging describes right ventricular function better than longitudinal displacement of the tricuspid ring. Heart. 2010; 96:281–288.8. Pirat B, McCulloch ML, Zoghbi WA. Evaluation of global and regional right ventricular systolic function in patients with pulmonary hypertension using a novel speckle tracking method. Am J Cardiol. 2006; 98:699–704.9. Jamal F, Bergerot C, Argaud L, Loufouat J, Ovize M. Longitudinal strain quantitates regional right ventricular contractile function. Am J Physiol Heart Circ Physiol. 2003; 285:H2842–H2847.10. Verhaert D, Mullens W, Borowski A, Popovic´ ZB, Curtin RJ, Thomas JD, Tang WH. Right ventricular response to intensive medical therapy in advanced decompensated heart failure. Circ Heart Fail. 2010; 3:340–346.11. Fine NM, Chen L, Bastiansen PM, Frantz RP, Pellikka PA, Oh JK, Kane GC. Outcome prediction by quantitative right ventricular function assessment in 575 subjects evaluated for pulmonary hypertension. Circ Cardiovasc Imaging. 2013; 6:711–721.12. Simonneau G, Galiè N, Rubin LJ, Langleben D, Seeger W, Domenighetti G, Gibbs S, Lebrec D, Speich R, Beghetti M, Rich S, Fishman A. Clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2004; 43:12 Suppl S. 5S–12S.13. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD, Spencer KT, Sutton MS, Stewart WJ. Chamber Quantification Writing Group. American Society of Echocardiography's Guidelines and Standards Committee. European Association of Echocardiography. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005; 18:1440–1463.14. Abbas AE, Fortuin FD, Schiller NB, Appleton CP, Moreno CA, Lester SJ. A simple method for noninvasive estimation of pulmonary vascular resistance. J Am Coll Cardiol. 2003; 41:1021–1027.15. Park JH, Negishi K, Kwon DH, Popovic ZB, Grimm RA, Marwick TH. Validation of global longitudinal strain and strain rate as reliable markers of right ventricular dysfunction: comparison with cardiac magnetic resonance and outcome. J Cardiovasc Ultrasound. 2014; 22:113–120.16. Pencina MJ, D'Agostino RB Sr, D'Agostino RB Jr, Vasan RS. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med. 2008; 27:157–172. discussion 207-1217. Harrell FE Jr, Lee KL, Mark DB. Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med. 1996; 15:361–387.18. Amundsen BH, Helle-Valle T, Edvardsen T, Torp H, Crosby J, Lyseggen E, Støylen A, Ihlen H, Lima JA, Smiseth OA, Slørdahl SA. Noninvasive myocardial strain measurement by speckle tracking echocardiography: validation against sonomicrometry and tagged magnetic resonance imaging. J Am Coll Cardiol. 2006; 47:789–793.19. Toyoda T, Baba H, Akasaka T, Akiyama M, Neishi Y, Tomita J, Sukmawan R, Koyama Y, Watanabe N, Tamano S, Shinomura R, Komuro I, Yoshida K. Assessment of regional myocardial strain by a novel automated tracking system from digital image files. J Am Soc Echocardiogr. 2004; 17:1234–1238.20. Thomas JD, Popovic´ ZB. Assessment of left ventricular function by cardiac ultrasound. J Am Coll Cardiol. 2006; 48:2012–2025.21. Geyer H, Caracciolo G, Abe H, Wilansky S, Carerj S, Gentile F, Nesser HJ, Khandheria B, Narula J, Sengupta PP. Assessment of myocardial mechanics using speckle tracking echocardiography: fundamentals and clinical applications. J Am Soc Echocardiogr. 2010; 23:351–369. quiz 453-5.22. Nahum J, Bensaid A, Dussault C, Macron L, Clémence D, Bouhemad B, Monin JL, Rande JL, Gueret P, Lim P. Impact of longitudinal myocardial deformation on the prognosis of chronic heart failure patients. Circ Cardiovasc Imaging. 2010; 3:249–256.23. Puwanant S, Park M, Popovic´ ZB, Tang WH, Farha S, George D, Sharp J, Puntawangkoon J, Loyd JE, Erzurum SC, Thomas JD. Ventricular geometry, strain, and rotational mechanics in pulmonary hypertension. Circulation. 2010; 121:259–266.24. Park JH, Kusunose K, Motoki H, Kwon DH, Grimm RA, Griffin BP, Marwick TH, Popovic´ ZB. Assessment of Right Ventricular Longitudinal Strain in Patients with Ischemic Cardiomyopathy: Head-to-Head Comparison between Two-Dimensional Speckle-Based Strain and Velocity Vector Imaging Using Volumetric Assessment by Cardiac Magnetic Resonance as a "Gold Standard". Echocardiography. 2014; 09. 18. [Epub].DOI: 10.1111/echo.12740.25. Bristow MR, Zisman LS, Lowes BD, Abraham WT, Badesch DB, Groves BM, Voelkel NF, Lynch DM, Quaife RA. The pressure-overloaded right ventricle in pulmonary hypertension. Chest. 1998; 114:1 Suppl. 101S–106S.26. Sachdev A, Villarraga HR, Frantz RP, McGoon MD, Hsiao JF, Maalouf JF, Ammash NM, McCully RB, Miller FA, Pellikka PA, Oh JK, Kane GC. Right ventricular strain for prediction of survival in patients with pulmonary arterial hypertension. Chest. 2011; 139:1299–1309.27. Bove AA, Santamore WP. Ventricular interdependence. Prog Cardiovasc Dis. 1981; 23:365–388.28. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982; 143:29–36.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Speckle Tracking Imaging in Patients with Pulmonary Hypertension
- Right Ventricular Longitudinal Strain: A Target Indicator in the Treatment of Pulmonary Arterial Hypertension
- Reduced Longitudinal Function in Chronic Aortic Regurgitation
- Application of Global Longitudinal Strain as a Parameter of Left Ventricular Systolic Function in Echocardiography
- A Case of Ascites and Extensive Abdominal Distension Caused by Reversible Pulmonary Arterial Hypertension Associated with Graves' Disease
