Multilocular developmental salivary gland defect
- Affiliations
-
- 1Department of Oral and Maxillofacial Radiology and Oral Biology Research Institute, School of Dentistry, Chosun University, Gwangju, Korea. hidds@chosun.ac.kr
- KMID: 1806794
- DOI: http://doi.org/10.5624/isd.2012.42.4.261
Abstract
- Developmental salivary gland defect is a bone depression on the lingual surface of the mandible containing salivary gland or fatty soft tissue. The most common location is within the submandibular gland fossa and often close to the inferior border of the mandible. This defect is asymptomatic and generally discovered only incidentally during radiographic examination of the area. This defect also appears as a well-defined, corticated, unilocular radiolucency below the mandibular canal. Although it is not uncommon for this defect to appear as a round or ovoid radiolucency, multilocular radiolucency of these defects is relatively rare. This report presents a case of a developmental salivary gland defect with multilocular radiolucency in a male patient.
MeSH Terms
Figure
-

Fig. 1 Panoramic radiograph reveals a well-defined multilocular radiolucent area beneath the mandibular canal at the root of the second molar tooth.
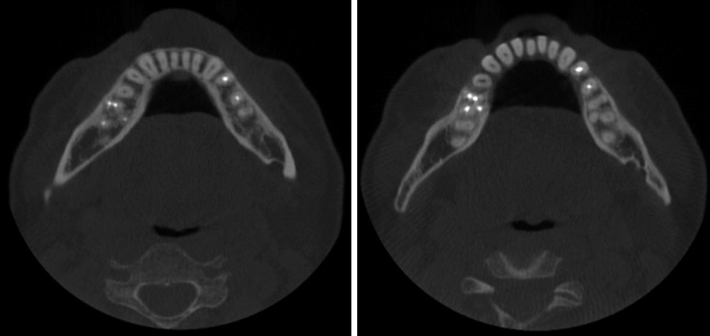
Fig. 2 Axial CBCT images show a lingual bony defect located at the lingual side of the mandibular canal.

Fig. 3 Coronal CBCT images show a lobulated bony defect below the mandibular canal.

Fig. 4 Para-sagittal CBCT image shows three lobulated radiolucencies with radiopaque margins between the mandibular canal and the inferior border of the mandibular canal.
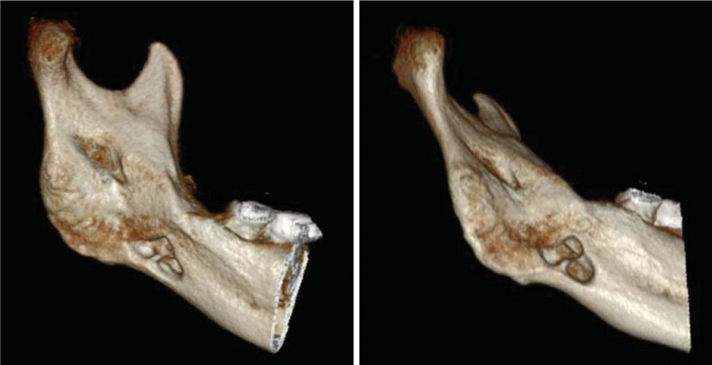
Fig. 5 Three-dimensional CBCT images reveal a bony defect extending from the medial surface of the mandible.
Cited by 1 articles
-
Developmental salivary gland depression in the ascending mandibular ramus: A cone-beam computed tomography study
Christine A. Chen, Yoonhee Ahn, Scott Odell, Mel Mupparapu, David Mattew Graham
Imaging Sci Dent. 2016;46(3):223-227. doi: 10.5624/isd.2016.46.3.223.
Reference
-
1. Stafne EC. Bone cavities situated near the angle of the mandible. J Am Dent Assoc. 1942. 29:1969–1972.
Article2. Philipsen HP, Takata T, Reichart PA, Sato S, Suei Y. Lingual and buccal mandibular bone depressions: a review based on 583 cases from a world-wide literature survey, including 69 new cases from Japan. Dentomaxillofac Radiol. 2002. 31:281–290.
Article3. Kim HK, Kim JS, Kim JD. Developmental salivary gland defect. Literatures review and case analysis of 12 cases. Korean J Oral Maxillofac Radiol. 2006. 36:81–88.4. Etöz M, Etöz OA, Sahman H, Sekerci AE, Polat HB. An unusual case of multilocular Stafne bone cavity. Dentomaxillofac Radiol. 2012. 41:75–78.
Article5. White SC, Pharoah MJ. Oral Radiology; principles and Interpretation. 2009. 6th ed. St. Louis: Mosby Inc;574.6. Nah KS, Jung YH, Cho BH. Unusual Stafne bone cavity mimicking infected cyst or neural origin tumor. Korean J Oral Maxillofac Radiol. 2007. 37:221–223.7. Shimizu M, Osa N, Okamura K, Yoshiura K. CT analysis of the Stafne's bone defects of the mandible. Dentomaxillofac Radiol. 2006. 35:95–102.
Article8. Minowa K, Inoue N, Sawamura T, Matsuda A, Totsuka Y, Nakamura M. Evaluation of static bone cavities with CT and MRI. Dentomaxillofac Radiol. 2003. 32:2–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Developmental salivary gland defect with extra-osseous course of the inferior alveolar nerve
- Developmental salivary gland defect: Literatures review and case analysis of 12 cases
- Clinical Experience in Reconstruction of the Posterior Lingual Mandibular Bony Defect
- Salivary Duct Carcinoma: 2 Case Reports
- Multiple sialolithiasis in sublingual gland: report of a case
