Psoas and Thigh Abscess Caused by Perforated Retrocecal Appendicitis: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, College of Medicine, Chungbuk National University, Cheongju, Korea. hyunchuls@chungbuk.ac.kr
- KMID: 1800392
- DOI: http://doi.org/10.4184/jkss.2015.22.1.31
Abstract
- STUDY DESIGN: A case report.
SUMMARY OF LITERATURE REVIEW: The symptoms of psoas abscess are fever, low back pain, and spasm of the psoas muscle.
OBJECTIVES
To report a case of psoas and thigh abscess caused by ruptured appendicitis.
MATERIALS AND METHODS
A 53- year old male patient visited the complaining of fever, low back pain and thigh pain. Imaging studies revealed psoas abscess and thigh abscess, accompanied by ruptured appendicitis. Therefore, surgical treatment with percutaneous drainage was performed.
RESULTS
The patient recovered and returned to his normal life after 2 months.
CONCLUSIONS
It is necessary to identify the cause of the infection using physical examination as well as abdominal and pelvis computed tomography when a patient has fever, psoas abscess and thigh abscess. It is also important to be aware that the cause of psoas abscess may also be gastrointestinal tract disease with non specific symptoms.
Keyword
MeSH Terms
Figure
-
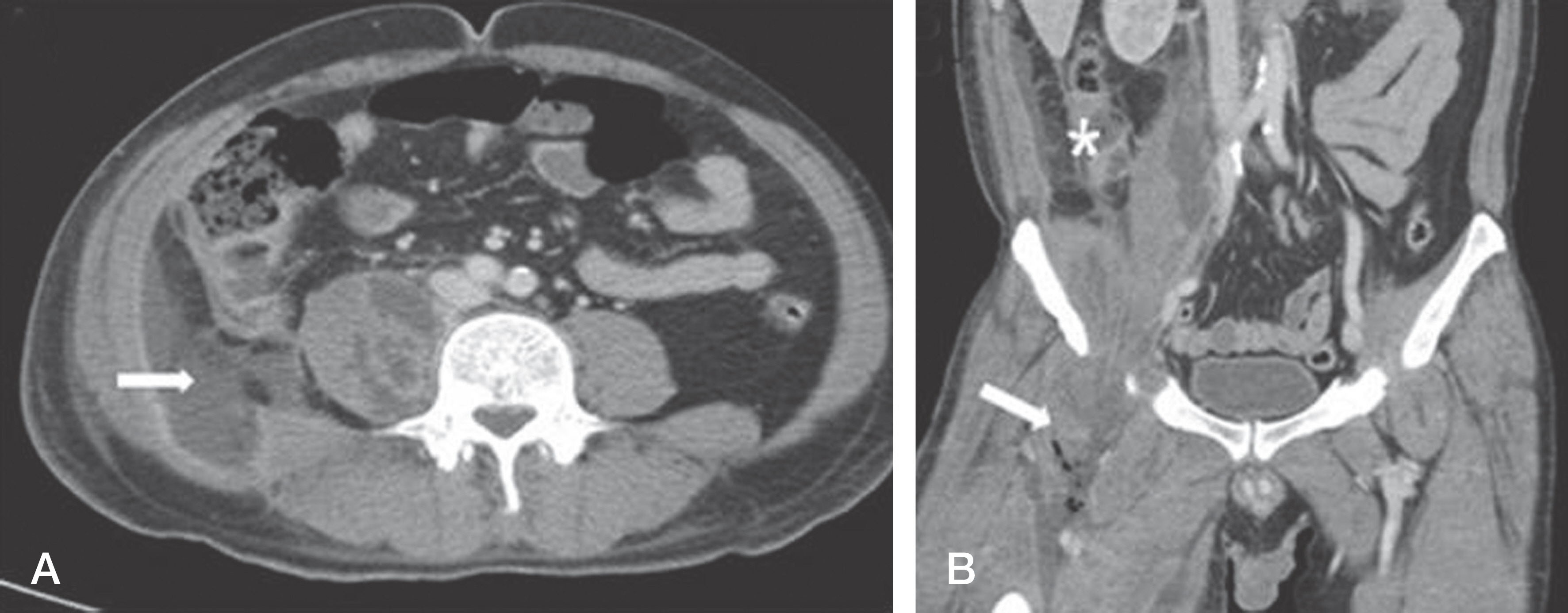
Fig. 1. (A) Axial contrast-enhanced CT scan shows multiple septated abscess in the right psoas muscle larger than left sided, and appendicitis, with leakage between the appendix and retroperotoneal fluid collection.(white arrow) (B) Reconstructed coronal contrast-enhanced CT scan shows dissection of the abscesses in the right thigh via the femoral canal, and shows gas containing abscesses in the right thigh.(white arrow) and heterogenous hypodense lesion with enhanced peripheral rim around appendix (asetrisk).

Fig. 2. After extensive surgical debridement and hemicolectomy, a percutaneous drainage catheter (arrow) was introduced into the right psoas muscle, and the same procedure (arrow) was performed for the right thigh.
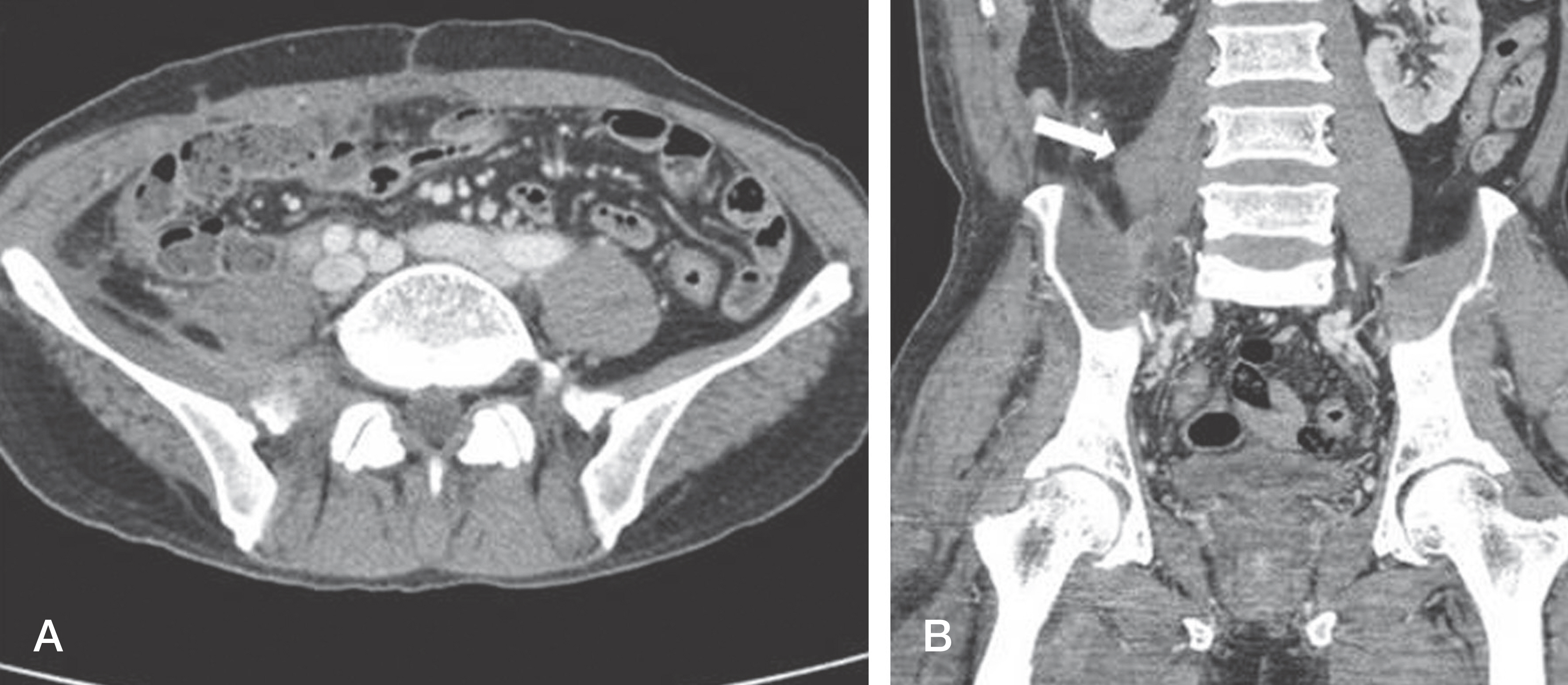
Fig. 3. (A) Three-month followup axial contrast-enhanced CT scan shows complete resolution (B) Reconstructed coronal contrast-enhanced CT scan also shows resolution. However irregular psoas muscle margine is noted (arrow).
Reference
-
1. Thongngarm T, McMurray RW. Primary psoa abscess. Ann Rheum Dis. 2001; 60:173–4.2. Haiart DC, Stevenson P, Hartley RC. Leg pain: an uncom-mon presentation of perforated diverticular disease. J R Coll Surg Edinb. 1989; 34:17–20.3. Haaga RJ, Alfidi RJ, Cooperman AM, et al. Definitive treatment of a large pyogenic liver abscess with CT guidance. Cleve Clin Q. 1976; 43:85–8.
Article4. Kim S, Lim HK, Lee JY, Lee J, Kim MJ, Lee AS. Ascending retrocecal appendicitis: clinical and computed tomographic findings. J Comput Assist Tomogr. 2006; 30:772–6.5. Taiwo B. Psoas abscess: a primer for the internist. South Med J. 2001; 94:2–5.6. An KC, Kim CW, Min YK. Clinical Availability, Diagnosis and Treatment of the Primary Psoas Muscle Abscess. J Korean Soc Spine Surg. 2010; 17:191–7.
Article7. Benoist S, Panis Y, Pannegeon V, et al. Can failure of percutaneous drainage of postoperative abdominal abscesses be predicted? Am J Surg. 2002; 184:148–53.
Article8. Hsieh CH, Wang YC, Yang HR, Chung PK, Jeng LB, Chen RJ. Extensive retroperitoneal and right thigh abscess in a patient with ruptured retrocecal appendicitis: an extremely fulminant form of a common disease. World J Gastroen-terol. 2006; 12:496–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Recurrent Psoas Abscess Caused by Two Different Pathogens: A Case Report
- Right thigh necrotizing fasciitis induced by perforated appendicitis
- Psoas Abscess Complicated from Psoas Compartment Block: A case report
- Primary Psoas Abscess: A Case Report
- A Case of Pelvic Abscess Due to the Perforated Appendicitis
