Screening for variations in anterior digastric musculature prior to correction of post-traumatic anterior open bite by injection of botulinum toxin type A: a technical note
- Affiliations
-
- 1Department of Natural Sciences and Mathematics, West Liberty University, West Liberty, WV, USA. mzdilla@westliberty.ed
- KMID: 1797848
- DOI: http://doi.org/10.5125/jkaoms.2015.41.3.165
Abstract
- It has recently been reported that long-standing post-traumatic open bite can be successfully corrected with botulinum toxin type A (BTX-A) injection into the anterior belly of the digastric muscle (ABDM). The report documented an individual with bilaterally symmetrical and otherwise unremarkable anterior digastric musculature. However, the existence of variant anterior digastric musculature is common and may complicate the management of anterior open bite with BTX-A injection. Screening for variant ABDM can be accomplished via ultrasound, computed tomography, and magnetic resonance imaging. Screening for variant ABDM should be performed prior to BTX-A injection in order to account for musculature that may exert undesired forces, such as inferolateral deviation, on the anterior mandible in patients with anterior open bite.
MeSH Terms
Figure
-
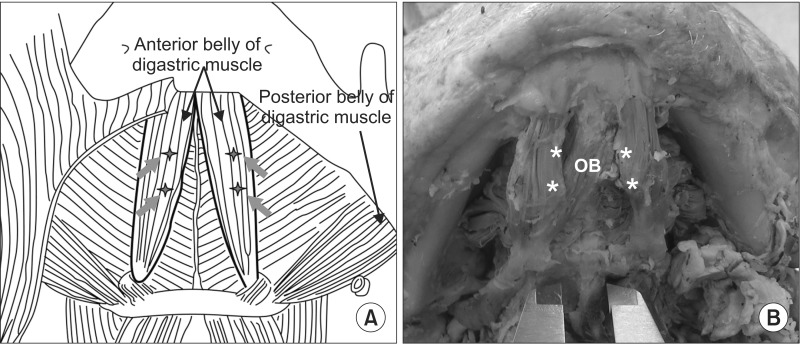
Fig. 1 Side-by-side comparison between normal and variant anterior digastric musculature with regard to botulinum toxin type A (BTX-A) injection sites. A. The line drawing from Seok et al.1, illustrating the BTX-A injection sites in bilaterally symmetrical anterior digastric muscle bellies (starburst with arrow: injection site). Image from the article of Seok et al. (J Korean Assoc Oral Maxillofac Surg 2013;39:188-92)1. B. A cadaveric example of an accessory oblique anterior digastric muscle belly crossing from the left digastric fossa of the mandible to the right intermediate tendon of the right digastric muscle that may complicate BTX-A injection for the correction of posttraumatic anterior open bite. Note that no injection site corresponding to those in Fig. 1. A is located on the accessory oblique digastric belly. (OB: oblique belly of the anterior digastric muscle, asterisk: injection site that correspond to those in Fig. 1. A). Image modified from the article of Zdilla et al. (J Surg Case Rep 2014. doi: 10.1093/jscr/rju131)7.
Reference
-
1. Seok H, Park YT, Kim SG, Park YW. Correction of post-traumatic anterior open bite by injection of botulinum toxin type A into the anterior belly of the digastric muscle: case report. J Korean Assoc Oral Maxillofac Surg. 2013; 39:188–192. PMID: 24471041.
Article2. Haskell R. Applied surgical anatomy. In : Williams JL, Rowe NL, editors. Rowe and Williams' maxillofacial injuries. 2nd ed. Edinburgh: Churchill Livingstone;1994. p. 12–14.3. Ozgur Z, Govsa F, Celik S, Ozgur T. An unreported anatomical finding: unusual insertions of the stylohyoid and digastric muscles. Surg Radiol Anat. 2010; 32:513–517. PMID: 19763380.
Article4. Sargon MF, Onderoğlu S, Sürücü HS, Bayramoğlu A, Demiryürek DD, Oztürk H. Anatomic study of complex anomalies of the digastric muscle and review of the literature. Okajimas Folia Anat Jpn. 1999; 75:305–313. PMID: 10217948.
Article5. Ozgur Z, Govsa F, Ozgur T. Bilateral quadrification of the anterior digastric muscles with variations of the median accessory digastric muscles. J Craniofac Surg. 2007; 18:773–775. PMID: 17667663.
Article6. Zdilla MJ, Soloninka HJ, Lambert HW. A fractal anterior digastric: a case report with surgical implications. Int J Anat Var. 2014; 7:106–108.7. Zdilla MJ, Soloninka HJ, Lambert HW. Unilateral duplication of the anterior digastric muscle belly: a case report with implications for surgeries of the submental region. J Surg Case Rep. 2014; DOI: 10.1093/jscr/rju131.
Article8. Harvey JA, Call Z, Peterson K, Wisco JJ. Weave pattern of accessory heads to the anterior digastric muscle. Surg Radiol Anat. 2014; [Epub ahead of print].
Article9. Klein AW. Complications, adverse reactions, and insights with the use of botulinum toxin. Dermatol Surg. 2003; 29:549–556. PMID: 12752527.
Article10. Alam M, Dover JS, Arndt KA. Pain associated with injection of botulinum A exotoxin reconstituted using isotonic sodium chloride with and without preservative: a double-blind, randomized controlled trial. Arch Dermatol. 2002; 138:510–514. PMID: 11939813.11. Walker TJ, Dayan SH. Comparison and overview of currently available neurotoxins. J Clin Aesthet Dermatol. 2014; 7:31–39. PMID: 24587850.12. Muraki AS, Mancuso AA, Harnsberger HR, Johnson LP, Meads GB. CT of the oropharynx, tongue base, and floor of the mouth: normal anatomy and range of variations, and applications in staging carcinoma. Radiology. 1983; 148:725–731. PMID: 6878693.
Article13. Larsson SG, Lufkin RB. Anomalies of digastric muscles: CT and MR demonstration. J Comput Assist Tomogr. 1987; 11:422–425. PMID: 3571582.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Correction of post-traumatic anterior open bite by injection of botulinum toxin type A into the anterior belly of the digastric muscle: case report
- Botulinum toxin-A injection into the anterior belly of the digastric muscle for the prevention of post-operative open bite in class II malocclusions: a case report and literature review
- The Change of the Maximal Bite-force after Botulinum Toxin A Injection for Lower Face Contouring
- Anterior open bite with temporomandibular disorders treated with intermaxillary traction using skeletal anchorage system
- Botulinum toxin A injection into the anterior belly of the digastric muscle increased the posterior width of the maxillary arch in developing rats
