Lemmel's Syndrome, an Unusual Cause of Abdominal Pain and Jaundice by Impacted Intradiverticular Enterolith: Case Report
- Affiliations
-
- 1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. sean4h@korea.ac.kr
- KMID: 1796954
- DOI: http://doi.org/10.3346/jkms.2014.29.6.874
Abstract
- Duodenal diverticula are detected in up to 27% of patients undergoing upper gastrointestinal tract evaluation with periampullary diverticula (PAD) being the most common type. Although PAD usually do not cause symptoms, it can serve as a source of obstructive jaundice even when choledocholithiasis or tumor is not present. This duodenal diverticulum obstructive jaundice syndrome is called Lemmel's syndrome. An 81-yr-old woman came to the emergency room with obstructive jaundice and cholangitis. Abdominal CT scan revealed stony opacity on distal CBD with CBD dilatation. ERCP was performed to remove the stone. However, the stone was not located in the CBD but rather inside the PAD. After removal of the enterolith within the PAD, all her symptoms resolved. Recognition of this condition is important since misdiagnosis could lead to mismanagement and therapeutic delay. Lemmel's syndrome should always be included as one of the differential diagnosis of obstructive jaundice when PAD are present.
MeSH Terms
-
Abdominal Pain
Aged, 80 and over
Cholangiopancreatography, Endoscopic Retrograde
Cholangiopancreatography, Magnetic Resonance
Cholangitis/complications
Diverticulum
Duodenal Diseases/complications/*diagnosis
Female
Fluoroscopy
Gallstones/diagnosis/therapy
Humans
Jaundice, Obstructive/*complications
Tomography, X-Ray Computed
Figure
-
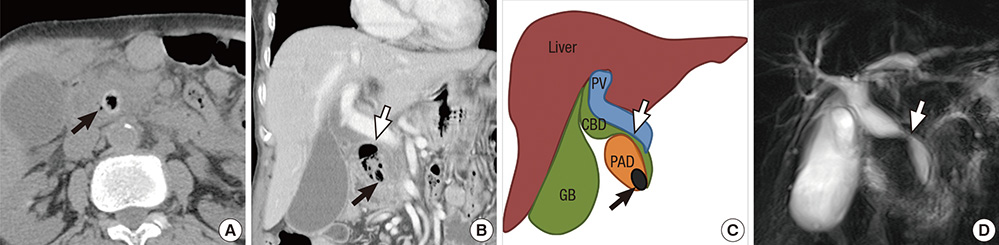
Fig. 1 Computed tomography (CT) and magnetic resonance cholangiopancreatography (MRCP) findings of the biliary tract. On axial CT scan, a high attenuated stone density with internal air (black arrow) is seen on distal common bile duct (CBD) (A). However, coronal reconstructed image shows that the stone (black arrow) is not located in the CBD but within the periampullary diverticulum that is filled with air and debris along with mid CBD stricture (white arrow) (B). This finding is depicted in line art to better delineate the anatomical relationship (C). Absence of CBD stone and mid CBD stricture is also demonstrated on MRCP image (D).
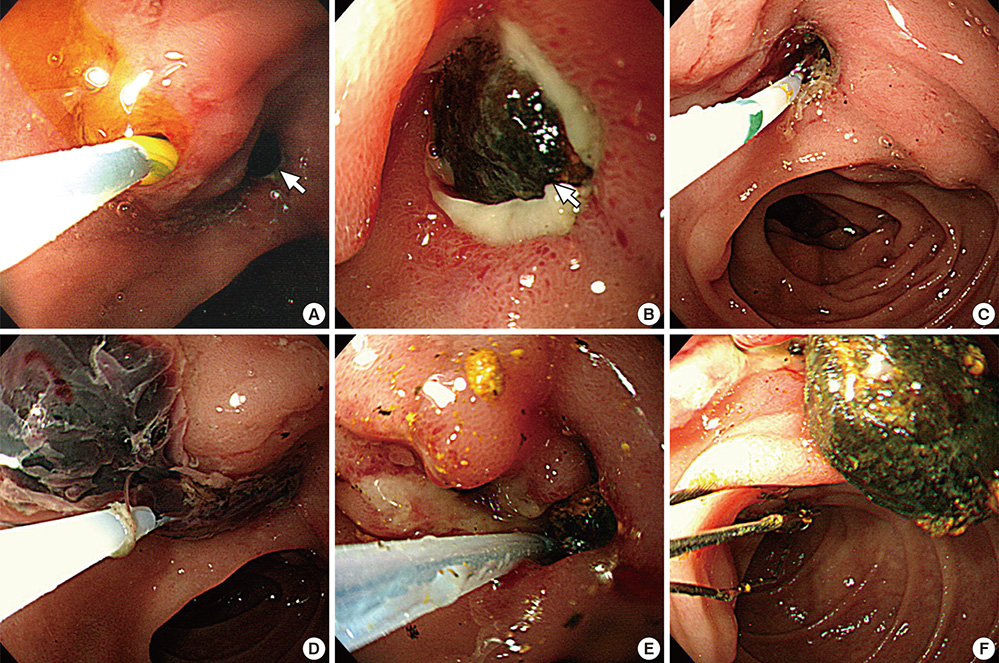
Fig. 2 Endoscopic retrograde cholangiopancreatographic findings of enterolith within the periampullary diverticulum (PAD) and its removal. A dark brown pigment stone (white arrow) is seen impacted at the orifice of the PAD (A, B). When the stone is pushed upward into the PAD (C), old blood clots is seen gushing out from the PAD orifice (D). The enterolith within the PAD is being fragmented and removed with Dormia basket (E, F).
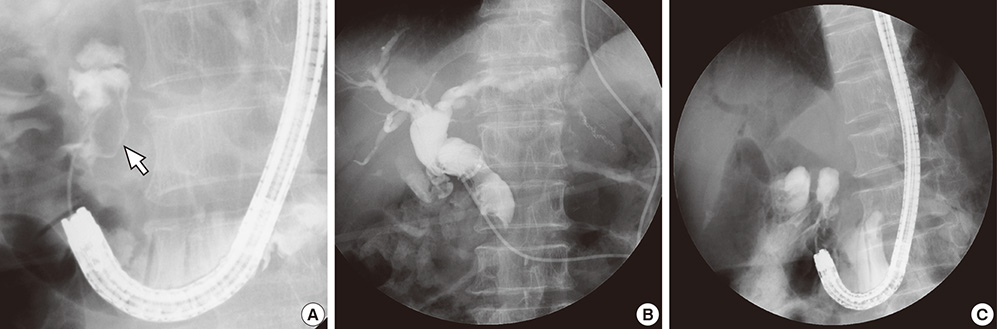
Fig. 3 Fluoroscopic images. When dye is injected into the PAD, an ovoid shaped filling defect (white arrow) can be seen (A). Endoscopic nasobiliary drainage tubogram obtained after decompression of the PAD demonstrates resolved extrinsic compression (B). After completion of enterolith removal, filling defect is no longer seen within the PAD (C).

Fig. 4 Removal of common bile duct (CBD) stone. Follow-up computed tomography scan taken about 6 months after enterolith removal shows an ovoid stone (white arrow) within the CBD (A). CBD stone (white arrow) removed by Dormia basket (B) proved to be brown pigment sludge stone (C).
Reference
-
1. Lobo DN, Balfour TW, Iftikhar SY, Rowlands BJ. Periampullary diverticula and pancreaticobiliary disease. Br J Surg. 1999; 86:588–597.2. Lemmel G. Die Klinische Bedeutung der Duodenal Divertikel. Arch Verdauungskrht. 1934; 46:59–70.3. Chomel JB. Report of a case of duodenal diverticulum containing gallstones. Histoire Acad R Sci Paris. 1710; 48–50.4. Manabe T, Yu GS. Duodenal diverticulum causing intermittent-persistent cholestasis: associated with papillitis chronica fibrosa. N Y State J Med. 1977; 77:2132–2136.5. Tomita R, Tanjoh K. Endoscopic manometry of the sphincter of Oddi in patients with Lemmel's syndrome. Surg Today. 1998; 28:258–261.6. Rouet J, Gaujoux S, Ronot M, Palazzo M, Cauchy F, Vilgrain V, Belghiti J, O'Toole D, Sauvanet A. Lemmel's syndrome as a rare cause of obstructive jaundice. Clin Res Hepatol Gastroenterol. 2012; 36:628–631.7. Nishida K, Kato M, Higashijima M, Takagi K, Akashi R. A case of Lemmel's syndrome caused by a large diverticular enterolith at the peripapillary portion of the duodenum. Nihon Ronen Igakkai Zasshi. 1995; 32:825–829.8. Shocket E, Simon SA. Small bowel obstruction due to enterolith (bezoar) formed in a duodenal diverticulum: a case report and review of the literature. Am J Gastroenterol. 1982; 77:621–624.9. Tham TC, Kelly M. Association of periampullary duodenal diverticula with bile duct stones and with technical success of endoscopic retrograde cholangiopancreatography. Endoscopy. 2004; 36:1050–1053.10. Lee JH, Lee JS, Kim HW, Bae SM, Kim SH, Kang DH, Song CS, Song GA, Cho M, Yang US. Association of periampullary diverticula with primary choledocholithiasis. Korean J Gastroenterol. 1999; 33:252–257.11. Skar V, Skar AG, Bratlie J, Osnes M. Beta-glucuronidase activity in the bile of gallstone patients both with and without duodenal diverticula. Scand J Gastroenterol. 1989; 24:205–212.12. Macari M, Lazarus D, Israel G, Megibow A. Duodenal diverticula mimicking cystic neoplasms of the pancreas: CT and MR imaging findings in seven patients. AJR Am J Roentgenol. 2003; 180:195–199.13. Kim SY, Kim JN, Kwon SO, Cha IH, Ryu SH, Kim YS, Moon JS. A case of duodenal diverticulum mimicking a peripancreatic abscess. Korean J Med. 2013; 84:249–253.14. Nonaka T, Inamori M, Kessoku T, Ogawa Y, Imajyo K, Yanagisawa S, Shiba T, Sakaguchi T, Nakajima A, Maeda S, et al. Acute obstructive cholangitis caused by an enterolith in a duodenal diverticulum. Endoscopy. 2010; 42:E204–E205.15. Yoneyama F, Miyata K, Ohta H, Takeuchi E, Yamada T, Kobayashi Y. Excision of a juxtapapillary duodenal diverticulum causing biliary obstruction: report of three cases. J Hepatobiliary Pancreat Surg. 2004; 11:69–72.16. Chiang TH, Lee YC, Chiu HM, Huang SP, Lin JT, Wang HP. Endoscopic therapeutics for patients with cholangitis caused by the juxtapapillary duodenal diverticulum. Hepatogastroenterology. 2006; 53:501–505.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Electrohydraulic Lithotripsy of an Impacted Enterolith Causing Acute Afferent Loop Syndrome
- Percutaneous Cholangioscopic Lithotripsy for Afferent Loop Syndrome Caused by Enterolith Development after Roux-en-Y Hepaticojejunostomy: A Case Report
- A case report of impacted fecalith within mucosal pouch: an unusual cause of colocolic intussusception
- A Case Report of Agenesis of Gallbladder which was Diagnosed after an Emergent operation Due to Ostructive Jundice with Impacted CBD Stones
- A Case of Meckel's Enterolith
