Calcaneal Insufficiency Avulsion Fracture in a Well-Controlled Type 2 Diabetic Patient: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery and Traumatology, Cheju Halla General Hospital, Jeju, Korea. jtahnos@gmail.com
- 2Department of Pathology, Cheju Halla General Hospital, Jeju, Korea.
- KMID: 1794887
- DOI: http://doi.org/10.14193/jkfas.2015.19.2.73
Abstract
- The calcaneal insufficiency avulsion fracture usually occurs in an area of fused apophysis in adults without significant history of trauma or overuse activities. It is an uncommon injury which has been described in patients with complicated diabetes, Charcot neuroarthropathy, amyloidosis with neuropathy, severe osteoporosis, and other conditions. Discussion of the issue of fracture location is still not sufficient. We report on a case of a 50-year-old male who experienced a non-traumatic diabetic calcaneal insufficiency fracture. Intraoperatively, a biopsy specimen was obtained from the exposed fracture site for histological study. We assume that the calcaneal fused apophyseal line is the weak point of failure due to various incomplete mixtures of trabecular bone, woven bone, and cartilaginous tissues, and may fail when repeated tensile stress is imposed.
Keyword
MeSH Terms
Figure
-
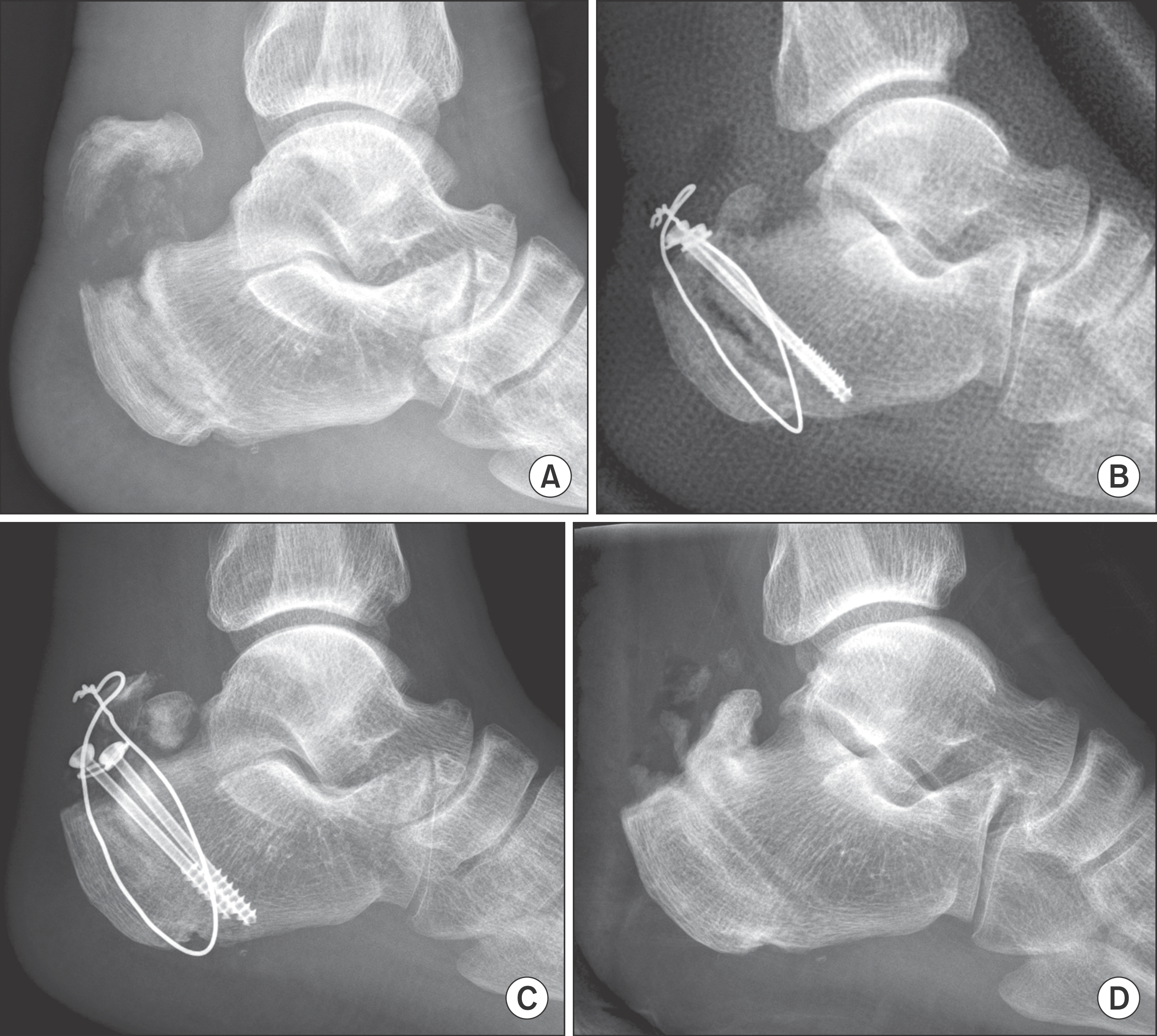
Figure 1. (A) Lateral radiograph shows about 1.5 cm upwardly displaced large avulsed fragment of calcaneal tubercle. Additionally, another sclerotic insufficiency avulsion fracture was combined which slipped upwardly parallel to the fused apophyseal line. (B) Postoperative radiograph shows reposition and fixation of fracture fragment with cerclage wiring and cannulated screws. (C) Postoperative four months radiograph shows re-displaced fracture fragment. (D) Final followup radiograph shows hardware removal.
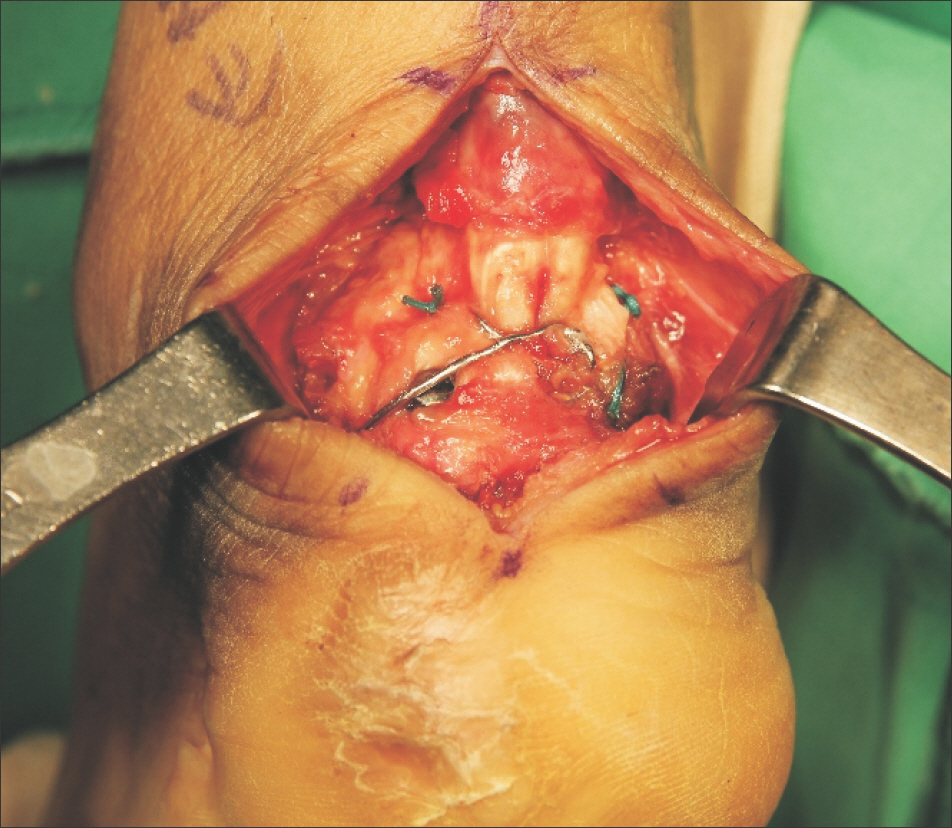
Figure 2. Fracture was fixed with cerclage wiring, cannulated screw and non-absorbable sutures.
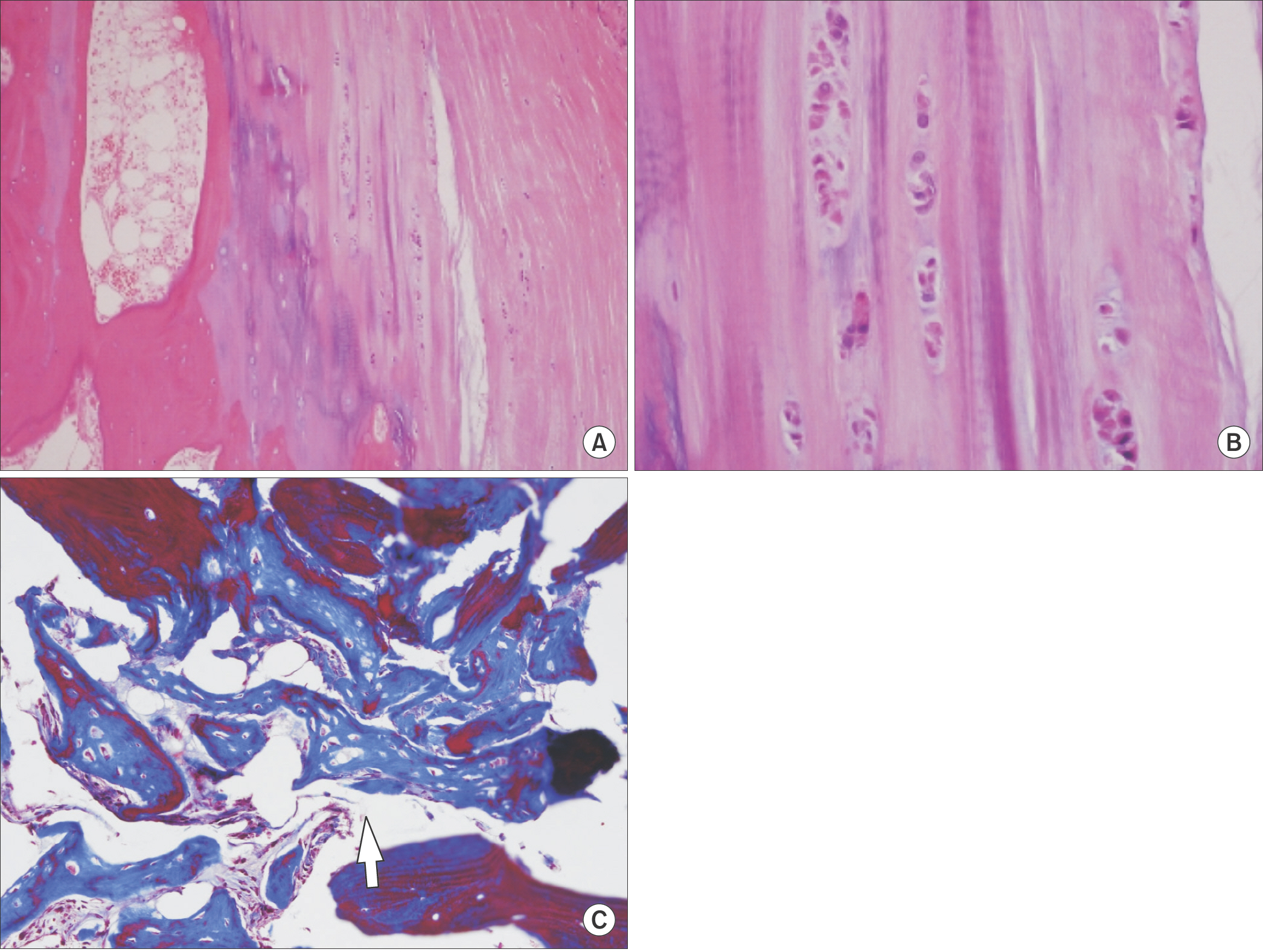
Figure 3. Histologic appearance of insufficiency fracture site is shown in low-power view (H&E stain, ×100; A), high-power view (H&E stain, ×400; B). Hyaline cartilaginous chondrocytes were arranged in small clusters surrounded by large amounts of moderately violescent stained matrix. (C) Abnormally oriented trabecular bone mixed with woven bones (arrow) are seen which is indicating various osteopathies and healing callus (Masson-Trichrome stain, ×200).
Cited by 1 articles
-
The Fate of Fracture Fragment in Diabetic Calcaneal Insufficiency Avulsion Fracture
Jeong-Hyun Park, Kwang-Rak Park, Gun-Hyun Park, Jaeho Cho
Korean J Phys Anthropol. 2018;31(2):65-70. doi: 10.11637/kjpa.2018.31.2.65.
Reference
-
1.Biehl WC 3rd., Morgan JM., Wagner FW Jr., Gabriel R. Neuropathic calcaneal tuberosity avulsion fractures. Clin Orthop Relat Res. 1993. 296:8–13.
Article2.Johnson JE., Thomson AB. Charcot neuroarthropathy of the foot: surgical aspects. Levin ME, O’Neal LW, Bowker JH, Pfeifer MA, editors. editors.Levin and O’Neal’s the diabetic foot. 7th ed.Philadelphia: Mosby/Elsevier;2008. p. 461–84.
Article3.Wren TA., Yerby SA., Beaupré GS., Carter DR. Influence of bone mineral density, age, and strain rate on the failure mode of human Achilles tendons. Clin Biomech (Bristol, Avon). 2001. 16:529–34.
Article4.Miki T., Miki T., Nishiyama A. Calcaneal stress fracture: an adverse event following total hip and total knee arthroplasty: a report of five cases. J Bone Joint Surg Am. 2014. 96:e9.5.Lee SM., Huh SW., Chung JW., Kim DW., Kim YJ., Rhee SK. Avulsion fracture of the calcaneal tuberosity: classification and its characteristics. Clin Orthop Surg. 2012. 4:134–8.
Article6.Grey A., Dalbeth N. Bone and rheumatic disorders in diabetes. Holt RIG, Cockram CS, Flyvbjerb A, Goldstein BJ, editors. editors.Textbook of diabetes. 4th ed.Chichester, West Sussex: Wiley-Blackwell;2010. p. 789–806.
Article7.Cundy TF., Edmonds ME., Watkins PJ. Osteopenia and metatarsal fractures in diabetic neuropathy. Diabet Med. 1985. 2:461–4.
Article8.Mascarenhas JV., Jude EB. Pathogenesis and medical management of diabetic Charcot neuroarthropathy. Med Clin North Am. 2013. 97:857–72.
Article9.Viguet-Carrin S., Garnero P., Delmas PD. The role of collagen in bone strength. Osteoporos Int. 2006. 17:319–36.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Fate of Fracture Fragment in Diabetic Calcaneal Insufficiency Avulsion Fracture
- Atraumatic Avulsion Fracture of Calcaneal Tuberosity in a Patient with Peripheral Neuropathy: A Case Report
- Avulsion Fracture of the Calcaneal Tuberosity: 2 Cases Report
- Natural History of the Calcaneal Avulsion Fracture in Neuropathic Arthropathy in a Young Diabetic Patient (A Case Report)
- Avulsion Fracture of Calcaneal Apophysis in an Adolescent Gymnast: A Case Report
