Early Experiences of Robotic-assisted Laparoscopic Liver Resection
- Affiliations
-
- 1Department of Surgery, Yonsei University College of Medicine, Seoul, Korea. kskim88@yuhs.ac
- KMID: 1793200
- DOI: http://doi.org/10.3349/ymj.2008.49.4.632
Abstract
- PURPOSE
The surgical robotic system is superior to traditional laparoscopy in regards to 3-dimensional images and better instrumentations. Robotic surgery for hepatic resection has not yet been extensively reported. PATIENTS and METHODS: Between March and May 2007, we performed 3 robot-assisted left lateral sectionectomies of the liver. Case 1 had a hepatocellular carcinoma (HCC), case 2 had colon cancer with liver metastasis, and case 3 had intrahepatic duct stones. RESULTS: All patients had successful operation and recovered without complications. Shorter length of hospital stays, earlier start of oral feeding and less amount of ascites were found. However, case 1 had recurrent HCC at 3 months after operation. CONCLUSION: Robotic-assisted liver surgery is still a new field in its developing stage. In patients with small malignant tumors and benign liver diseases, robotic-assisted laparoscopic resection is feasible and safe. Through experience, the use of robotics is expected to increase in the treatment of benign diseases and malignant neoplsms. However, careful patient selection is important and long-term outcomes need to be evaluated.
MeSH Terms
Figure
-
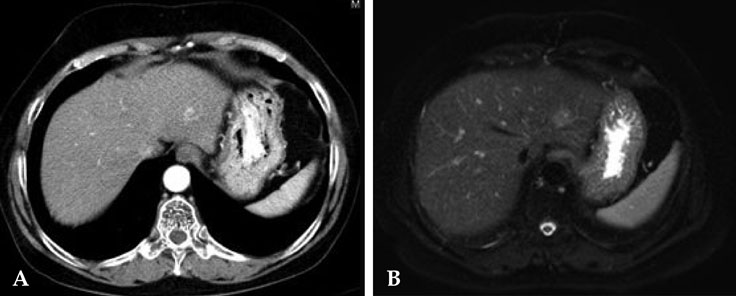
Fig. 1 CT (A) and MRI (B) show a 2 cm mass consistent with HCC in segment II. HCC, hepatocellular carcinoma.

Fig. 2 CT shows a hypodense, 1.5 cm mass (A) in segment III consistent with metastasis and an ulcerofungating mass (B) with minimal pericolic fat infiltration at the rectosigmoid junction.

Fig. 3 Precontrast CT shows IHD and CBD dilatation with several radiopaque stones in liver segment II (A) and a 6 mm calcified stone in the distal CBD (B). IHD, intrahepatic duct; CBD, common bile duct.
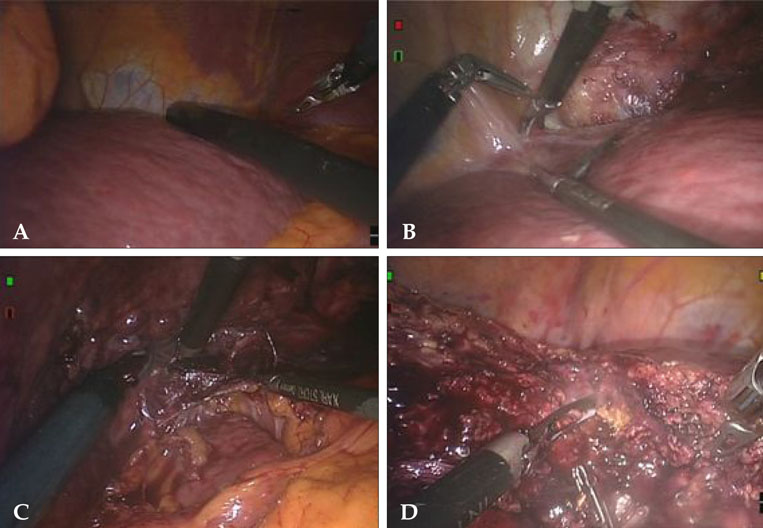
Fig. 4 Operative procedures. Intraoperative ultrasonography for detecting other lesions and determining resection margins (A). Dissection of falciform ligament and ligamentum venosum after detaching the left triangular ligament using a harmonic scalpel (B and C). Parenchymal dissection using a harmonic scalpel and electrocautery (D).

Fig. 5 Suture for Glissonian pedicle (A) and endo-GIA for division of hepatic vein (B).

Fig. 6 A 3-month follow-up CT showed multiple intrahepatic masses compatible with HCC with tumor thrombi in the main portal trunk (A). PET scan shows multiple strong F-18 FDG uptakes at the liver and pelvic bone (B and C). HCC, hepatocellular carcinoma; PET, positron emission tomography.
Cited by 4 articles
-
Robotic Colorectal Surgery
Seung Hyuk Baik
Yonsei Med J. 2008;49(6):891-896. doi: 10.3349/ymj.2008.49.6.891.Recent advances in hepatic resection and liver transplantation for hepatocellular carcinoma
Shin Hwang
J Korean Med Assoc. 2013;56(11):956-963. doi: 10.5124/jkma.2013.56.11.956.Efficacy and Safety of Robotic Procedures Performed Using the da Vinci Robotic Surgical System at a Single Institute in Korea: Experience with 10000 Cases
Dong Hoon Koh, Won Sik Jang, Jae Won Park, Won Sik Ham, Woong Kyu Han, Koon Ho Rha, Young Deuk Choi
Yonsei Med J. 2018;59(8):975-981. doi: 10.3349/ymj.2018.59.8.975.Total robotic right hepatectomy for multifocal hepatocellular carcinoma using vessel sealer
Peeyush Varshney, Vaibhav Kumar Varshney
Ann Hepatobiliary Pancreat Surg. 2023;27(1):95-101. doi: 10.14701/ahbps.22-036.
Reference
-
1. Hanly EJ, Talamini MA. Robotic abdominal surgery. Am J Surg. 2004. 188:4A Suppl. 19S–26S.
Article2. Vidovszky TJ, Smith W, Ghosh J, Ali MR. Robotic cholecystectomy: learning curve, advantages, and limitations. J Surg Res. 2006. 136:172–178.3. Hashizume M, Tsugawa K. Robotic surgery and cancer: the present state, problems and future vision. Jpn J Clin Oncol. 2004. 34:227–237.
Article4. D'Annibale A, Morpurgo E, Fiscon V, Trevisan P, Sovernigo G, Orsini C, et al. Robotic and laparoscopic surgery for treatment of colorectal disease. Dis Colon Rectum. 2004. 47:2162–2168.5. Camarillo DB, Krummel TM, Salisbury JK Jr. Robotic technology in surgery: past, present, and future. Am J Surg. 2004. 188:4A Suppl. 2S–15S.6. Nguyen MM, Das S. The evolution of robotic urologic surgery. Urol Clin North Am. 2004. 31:653–658. vii.
Article7. Lee YS, Han WK, Oh YT, Choi YD, Yang SC, Rha KH. Robot-assisted laparoscopic radical prostatectomy: four cases. Yonsei Med J. 2007. 48:341–346.8. Anvari M, Birch DW, Bamehriz F, Gryfe R, Chapman T. Robotic-assisted laparoscopic colorectal surgery. Surg Laparosc Endosc Percutan Tech. 2004. 14:311–315.
Article9. Talamini MA, Chapman S, Horgan S, Melvin WS. The Academic Robotics Group. A prospective analysis of 211 robotic-assisted surgical procedures. Surg Endosc. 2003. 17:1521–1524.10. Patel VR, Chammas MF Jr, Shah S. Robotic assisted laparoscopic radical prostatectomy: a review of the current state of affairs. Int J Clin Pract. 2007. 61:309–314.11. Simillis C, Constantinides VA, Tekkis PP, Darzi A, Lovegrove R, Jiao L, et al. Laparoscopic versus open hepatic resections for benign and malignant neoplasms-a meta-analysis. Surgery. 2007. 141:203–211.
Article12. Vibert E, Perniceni T, Levard H, Denet C, Shahri NK, Gayet B. Laparoscopic liver resection. Br J Surg. 2006. 93:67–72.
Article13. Chang S, Laurent A, Tayar C, Karoui M, Cherqui D. Laparoscopy as a routine approach for left lateral sectionectomy. Br J Surg. 2007. 94:58–63.
Article14. Santambrogio R, Opocher E, Ceretti AP, Barabino M, Costa M, Leone S, et al. Impact of intraoperative ultrasonography in laparoscopic liver surgery. Surg Endosc. 2007. 21:181–188.
Article15. Allardyce RA. Is the port site really at risk? Biology, mechanisms and prevention: a critical view. Aust N Z J Surg. 1999. 69:479–485.
Article16. Gutt CN, Kim ZG, Hollander D, Bruttel T, Lorenz M. CO2 environment influences the growth of cultured human cancer cells dependent on insufflation pressure. Surg Endosc. 2001. 15:314–318.
Article17. Takiguchi S, Matsuura N, Hamada Y, Taniguchi E, Sekimoto M, Tsujinaka M, et al. Influence of CO2 pneumoperitoneum during laparoscopic surgery on cancer cell growth. Surg Endosc. 2000. 14:41–44.
Article18. Nagasue N, Uchida M, Makino Y, Takemoto Y, Yamanoi A, Hayashi T, et al. Incidence and factors associated with intrahepatic recurrence following resection of hepatocellular carcinoma. Gastroenterology. 1993. 105:488–494.
Article19. Poon RT, Fan ST, Ng IO, Lo CM, Liu CL, Wong J. Different risk factors and prognosis for early and late intrahepatic recurrence after resection of hepatocellular carcinoma. Cancer. 2000. 89:500–507.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Robotic-assisted right hepatectomy via anterior approach for intrahepatic cholangiocarcinoma
- Initial Experience with Laparoscopic and DaVinci Robotic-assisted Liver Resection
- Current status of robotic surgery for liver transplantation
- Robotic-assisted resection of proximal jejunal ischemic stricture and intracorporeal robot-sewn anastomosis
- Simultaneous Laparoscopic Resection of Advanced Colorectal Cancer and Early Gastric Cancer
