Modified Mandibulotomy Technique to Reduce Postoperative Complications: 5-Year Results
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, College of Dentistry, Yonsei University, Seoul, Korea. omsnam@yuhs.ac
- 2Department of Otorhinolaryngology, Yonsei University College of Medicine, Seoul, Korea. eunchangmd@yuhs.ac
- KMID: 1793175
- DOI: http://doi.org/10.3349/ymj.2013.54.5.1248
Abstract
- PURPOSE
To review the 5-year outcomes of our modified mandibulotomy technique. Retrospective review of a tertiary level oral cancer center.
MATERIALS AND METHODS
During a 5-year period, 30 patients who had a uniform surgical technique consisting of a lower lip-splitting, modified stair-step osteotomy with thin saw blade and osteotome after plate-precontouring and combination fixation with monocortical osteosynthesis (miniplate) and bicortical osteosynthesis (maxiplate and bicortical screws), with at least 14 months postoperative follow-up, were selected and reviewed retrospectively.
RESULTS
There were 8 women and 22 men with an average age of 56.5 years. All the patients involved malignancies were squamous cell carcinoma. The main primary sites of the those who underwent a mandibulotomy were the tonsil, the base of tongue, the oral tongue, the retromolar pad area, and others. Others included buccal cheek, floor of mouth, and soft palate. 23 patients received postoperative radiation therapy, and among whom 8 patients also received chemotherapy. Total four (13%) mandibulotomy-related complications occurred, only two (6.7%) requiring additional operation under general anesthesia.
CONCLUSION
Our modified mandibulotomy meets the criteria for an ideal mandibulotomy technique relatively well because it requires no intermaxillary fixation, can precise preserve the occlusion in a precise way, allows early function, requires no secondary procedures, and has few complications.
MeSH Terms
Figure
-

Fig. 1 Schematic diagram of lingual osteotomy with an oscillating saw in the preconstruction phase of intentional fracture. Note that the osteotomy should be continued until the oscillating saw is as close to the outer surface of the lingual cortex as possible.
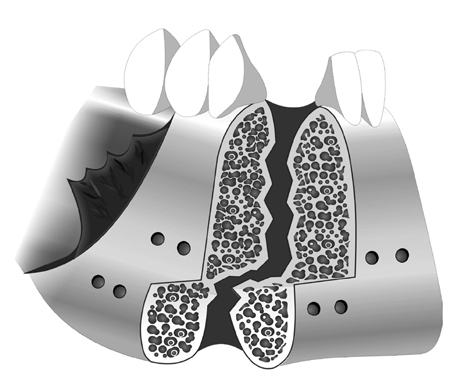
Fig. 2 Schematic diagram of bucco-lingual corticotomy. Note that the buccal corticotomy is completed with a saw and the lingual corticotomy with an osteotome following indentation of the lingual cortex with an oscillating saw. The inferior border of the mandible should be completely osteotomized to prevent undesirable splitting while malleting the osteotome due to the inferior border's thick cortex.
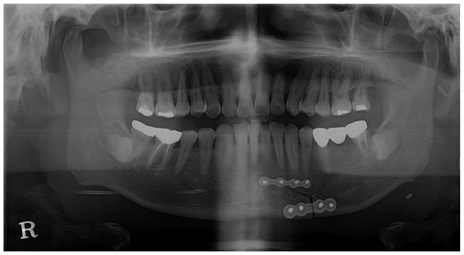
Fig. 3 Fixation using bicortical and monocortical plates and screws. Our modified technique does not require IMF or tooth extraction.
Cited by 1 articles
-
Guidelines for the Surgical Management of Oral Cancer: Korean Society of Thyroid-Head and Neck Surgery
Young-Hoon Joo, Jae-Keun Cho, Bon Seok Koo, Minsu Kwon, Seong Keun Kwon, Soon Young Kwon, Min-Su Kim, Jeong Kyu Kim, Heejin Kim, Innchul Nam, Jong-Lyel Roh, Young Min Park, Il-Seok Park, Jung Je Park, Sung-Chan Shin, Soon-Hyun Ahn, Seongjun Won, Chang Hwan Ryu, Tae Mi Yoon, Giljoon Lee, Doh Young Lee, Myung-Chul Lee, Joon Kyoo Lee, Jin Choon Lee, Jae-Yol Lim, Jae Won Chang, Jeon Yeob Jang, Man Ki Chung, Yuh-Seok Jung, Jae-Gu Cho, Yoon Seok Choi, Jeong-Seok Choi, Guk Haeng Lee, Phil-Sang Chung
Clin Exp Otorhinolaryngol. 2019;12(2):107-144. doi: 10.21053/ceo.2018.01816.
Reference
-
1. Butlin HT. Diseases of the tongue. London: Cassell;1885. p. 331.2. Martin H, Tollefsen HR, Gerold FP. Median labiomandibular glossotomy. Trotter's median (anterior) translingual pharyngotomy. Am J Surg. 1961; 102:753–759.3. McGregor IA, MacDonald DG. Mandibular osteotomy in the surgical approach to the oral cavity. Head Neck Surg. 1983; 5:457–462.
Article4. Davidson J, Freeman J, Birt D. Mandibulotomy in the irradiated patient. Arch Otolaryngol Head Neck Surg. 1989; 115:497–499.
Article5. Davidson J, Freeman J, Gullane P, Rotstein L, Birt D. Mandibulotomy and radical radiotherapy: compatible or not? J Otolaryngol. 1988; 17:279–281.6. McCann KJ, Irish JC, Gullane PJ, Holmes H, Brown DH, Rotstein L. Complications associated with rigid fixation of mandibulotomies. J Otolaryngol. 1994; 23:210–215.7. Spiro RH, Gerold FP, Strong EW. Mandibular "swing" approach for oral and oropharyngeal tumors. Head Neck Surg. 1981; 3:371–378.
Article8. Sullivan PK, Fabian R, Driscoll D. Mandibular osteotomies for tumor extirpation: the advantages of rigid fixation. Laryngoscope. 1992; 102:73–80.9. Shah JP, Kumaraswamy SV, Kulkarni V. Comparative evaluation of fixation methods after mandibulotomy for oropharyngeal tumors. Am J Surg. 1993; 166:431–434.
Article10. Singh AM, Bahadur S, Tandon DA, Pande RM. Anterior mandibulotomy for oral and oropharyngeal tumours. J Laryngol Otol. 1993; 107:316–319.
Article11. Altman K, Bailey BM. Non-union of mandibulotomy sites following irradiation for squamous cell carcinoma of the oral cavity. Br J Oral Maxillofac Surg. 1996; 34:62–65.
Article12. Amin MR, Deschler DG, Hayden RE. Straight midline mandibulotomy revisited. Laryngoscope. 1999; 109:1402–1405.
Article13. Aslan G, Kargi E, Görgü M, Erdoğan B, Kilinç H. Modified mandibulotomy approach to tumors of the oropharynx. Ann Plast Surg. 2001; 46:77–79.
Article14. Flood TR, Hislop WS. A modified surgical approach for parapharyngeal space tumours: use of the inverted 'L' osteotomy. Br J Oral Maxillofac Surg. 1991; 29:82–86.
Article15. Jungehuelsing M, Guntinas-Lichius O, Klussmann JP, Eckel HE, Stennert E. Modifications of the midline mandibulotomy for access to the parapharyngeal space. Laryngoscope. 2010; 120:1557–1562.
Article16. Sardi A, Walters PJ. Modified mandibular swing procedure for resection of carcinoma of the oropharynx. Head Neck. 1991; 13:394–397.
Article17. Cohen JI, Marentette LJ, Maisel RH. The mandibular swing stabilization of the midline mandibular osteotomy. Laryngoscope. 1988; 98:1139–1142.18. Carraway JH, McGregor IA. Restoration of mandibular continuity after symphyseal osteotomy. Br J Plast Surg. 1981; 34:392–394.
Article19. Dziegielewski PT, Mlynarek AM, Dimitry J, Harris JR, Seikaly H. The mandibulotomy: friend or foe? Safety outcomes and literature review. Laryngoscope. 2009; 119:2369–2375.
Article20. Kolokythas A, Eisele DW, El-Sayed I, Schmidt BL. Mandibular osteotomies for access to select parapharyngeal space neoplasms. Head Neck. 2009; 31:102–110.
Article21. Nam W, Kim HJ, Choi EC, Kim MK, Lee EW, Cha IH. Contributing factors to mandibulotomy complications: a retrospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 101:e65–e70.
Article22. Nam W, Kim HJ, Chung SW, Choi EC, Cha IH. Modified mandibulotomy technique to reposition the hemimandibular segments. J Oral Maxillofac Surg. 2007; 65:1433–1435.
Article23. Engroff SL, Blanchaert RH Jr, von Fraunhofer JA. Mandibulotomy fixation: a laboratory analysis. J Oral Maxillofac Surg. 2003; 61:1297–1301.
Article24. Dubner S, Spiro RH. Median mandibulotomy: a critical assessment. Head Neck. 1991; 13:389–393.
Article25. Dziegielewski PT, O'Connell DA, Rieger J, Harris JR, Seikaly H. The lip-splitting mandibulotomy: aesthetic and functional outcomes. Oral Oncol. 2010; 46:612–617.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Midline Mandibulotomy: Functional Outcomes
- Mandibulotomy, A Surgical approach for Oral cancer: Its Complications and contributing factors
- Clinical Evaluation between Mandibulotomy and Mandible Sparing Approaches in Oropharyngeal Cancer Operation and Reconstruction
- The Utility of Paramedian Mandibulotomy for Resection of Oral Cavity and Oropharynx Cancer
- Use of a Modified Ultrafiltration Technique during Aortic Valve Replacement Surgery on a Jehovah's Witness
