Acute Myocardial Infarction after Radiofrequency Catheter Ablation of Typical Atrial Flutter
- Affiliations
-
- 1Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 2Division of Cardiolgy, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. js58.kim@samsung.com
- KMID: 1789991
- DOI: http://doi.org/10.3346/jkms.2014.29.2.292
Abstract
- A 53-yr-old man underwent radiofrequency ablation to treat persistent atrial flutter. After the procedure, the chest pain was getting worse, and the electrocardiogram showed ST-segment elevation in inferior leads with reciprocal changes. Immediate coronary angiography showed total occlusion with thrombi at the distal portion of the right coronary artery, which was very close to the ablation site. Intervention with thrombus aspiration and balloon dilatation was successful, and the patient recovered without any kind of sequelae. Although the exact mechanism is obscure, the most likely explanation is a thermal injury to the vascular wall that ruptured into the lumen and formed thrombus. Vasospasm and thromboembolism can also be other possibilities. This case raise the alarm to cardiologists who perform radiofrequency ablation to treat various kinds of cardiac arrhythmias, in that myocardial infarction has been rarely considered one of the complications.
MeSH Terms
Figure
-
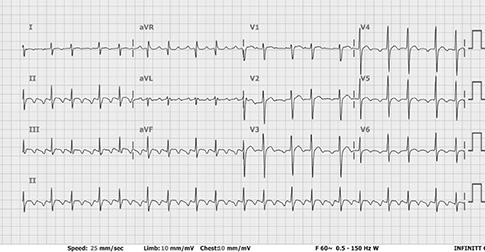
Fig. 1 Resting electrocardiography showed typical atrial flutter with 2:1 or 3:1 conduction before the radiofrequency ablation.
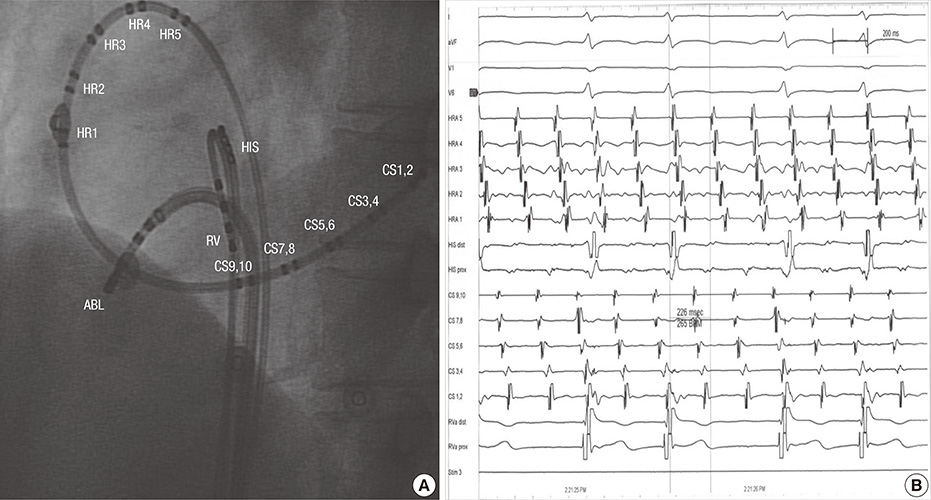
Fig. 2 Ablation of atrial flutter. (A) The fluoroscopic image, left anterior oblique, showing the position of ablation and diagnostic catheters. (B) Intracardiac electrogram showing typical counterclockwise atrial flutter. ABL, ablation; HIS, His bundle; CS, coronary sinus; RVA, right ventricular apex.
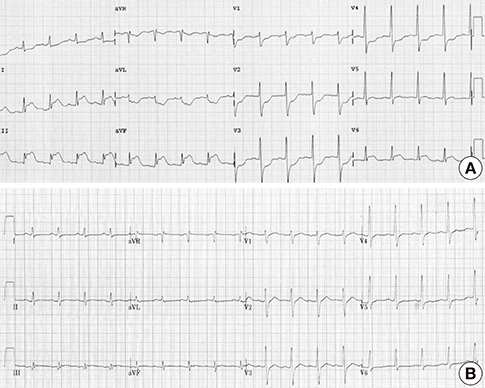
Fig. 3 Electrocardiograms. (A) Right after the radiofrequency ablation. Elevation of ST-segment in lead II, III, aVF and reciprocal change in the anterior precordial leads are noted. (B) After an hour of the primary coronary intervention. Previous ST-T changes disappeared.
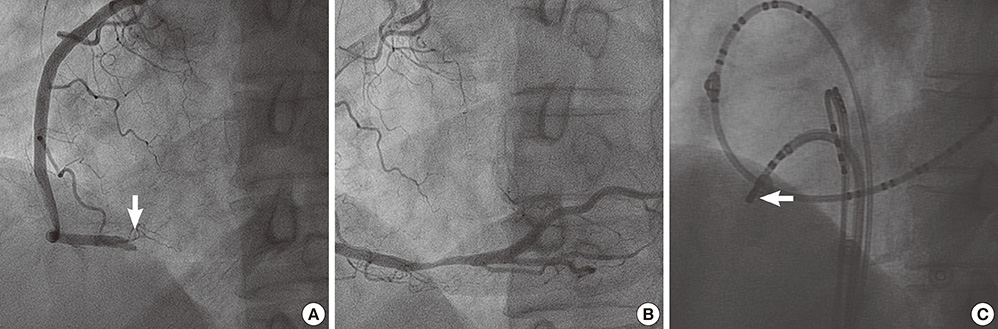
Fig. 4 Acute occlusion of right coronary artery. (A) Coronary angiography, right anterior oblique, showing total occlusion of at the distal portion of right coronary artery (arrow). (B) Revascularization after balloon angioplasty with resultant 20% residual stenosis. (C) The fluoroscopic image, left anterior oblique, showing the position of ablation catheter tip during radiofrequency ablation (arrow).
Reference
-
1. Weiss C, Becker J, Hoffmann M, Willems S. Can radiofrequency current isthmus ablation damage the right coronary artery? histopathological findings following the use of a long (8 mm) tip electrode. Pacing Clin Electrophysiol. 2002; 25:860–862.2. Sassone B, Leone O, Martinelli GN, Di Pasquale G. Acute myocardial infarction after radiofrequency catheter ablation of typical atrial flutter: histopathological findings and etiopathogenetic hypothesis. Ital Heart J. 2004; 5:403–407.3. Ouali S, Anselme F, Savouré A, Cribier A. Acute coronary occlusion during radiofrequency catheter ablation of typical atrial flutter. J Cardiovasc Electrophysiol. 2002; 13:1047–1049.4. Mykytsey A, Kehoe R, Bharati S, Maheshwari P, Halleran S, Krishnan K, Razminia M, Mina A, Trohman RG. Right coronary artery occlusion during RF ablation of typical atrial flutter. J Cardiovasc Electrophysiol. 2010; 21:818–821.5. Caldwell JC, Fath-Odoubadi F, Garratt CJ. Right coronary artery damage during cavotricuspid isthmus ablation. Pacing Clin Electrophysiol. 2010; 33:e110–e113.6. Al Aloul B, Sigurdsson G, Can I, Li JM, Dykoski R, Tholakanahalli VN. Proximity of right coronary artery to cavotricuspid isthmus as determined by computed tomography. Pacing Clin Electrophysiol. 2010; 33:1319–1323.7. Paul T, Bökenkamp R, Mahnert B, Trappe HJ. Coronary artery involvement early and late after radiofrequency current application in young pigs. Am Heart J. 1997; 133:436–440.8. Simon RD, Gill JS. Coronary ischemia induced by radiofrequency ablation in the left atrium. J Cardiovasc Electrophysiol. 2003; 14:186–190.9. Yamazaki K, Funayama N, Okabayashi H, Myojo T, Gima M, Tanaka H, Sakamoto N, Kikuchi K. Acute coronary syndrome due to coronary thrombus formed by severe coronary spasm: a case report. J Cardiol. 2007; 50:205–212.10. Taniguchi Y, Nakamura M, Suzuki T, Suzuki T, Aoki H, Fukami KI. A case of acute myocardial infarction: intracoronary thrombus formation at a previously provoked vasospasm site. Jpn Heart J. 2000; 41:761–766.11. Kadowaki K, Sato T, Abe Y, Yanagiya N, Kumagai T. A case of acute myocardial infarction following intracoronary thrombi caused by coronary artery spasm. Kokyu To Junkan. 1992; 40:705–708.12. Horimoto M, Takenaka T, Igarashi K, Fujiwara M, Batra S. Coronary spasm as a cause of coronary thrombosis and myocardial infarction. Jpn Heart J. 1993; 34:627–631.13. Hasegawa A, Horimoto M, Takenaka T, Igarashi K. Coronary spasm-induced acute myocardial infarction associated with intracoronary thrombosis. Kokyu To Junkan. 1992; 40:189–193.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management of Atrial Flutter
- Catheter Ablation of Atrial Flutter Using Radiofrequency Energy in a Child: A Case Report
- Radiofrequency Catheter Ablation in Patients with Atrial Flutter
- Cerebral Infarction After Radiofrequency Catheter Ablation in Patients With Paroxysmal Atrial Fibrillation
- Restoration of Atrial Mechanical Function after Successful Radio-Frequency Catheter Ablation of Atrial Flutter
