J Korean Med Sci.
2013 Apr;28(4):624-627. 10.3346/jkms.2013.28.4.624.
Spontaneous Healing of Gastric Perforation after Endoscopic Ligation for Gastric Varices
- Affiliations
-
- 1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Gachon University Gil Medical Center, Incheon, Korea. toptom@gilhospital.com
- KMID: 1786974
- DOI: http://doi.org/10.3346/jkms.2013.28.4.624
Abstract
- Endoscopic variceal ligation (EVL) can be performed as an optional therapy for gastric variceal bleeding if endoscopic sclerotherapy (ES) is not readily available or if practitioners lack experience. EVL using an endoscopic pneumo-activated ligating device was performed on a 53-year-old male patient with liver cirrhosis who presented with hematemesis. Follow-up esophagogastroduodenoscopy (EGD) performed two days after the EVL showed gastric perforation at the EVL-procedure site on the gastric fundus. However, the patient refused emergency surgery, and therefore received only supportive management, including intravenous antibiotics. EGD 10 days later showed healing of the perforation site. This is the first report of a case of gastric variceal bleeding with development of a gastric perforation soon after EVL, which showed complete recovery with conservative therapy and without surgical intervention.
Keyword
MeSH Terms
Figure
-
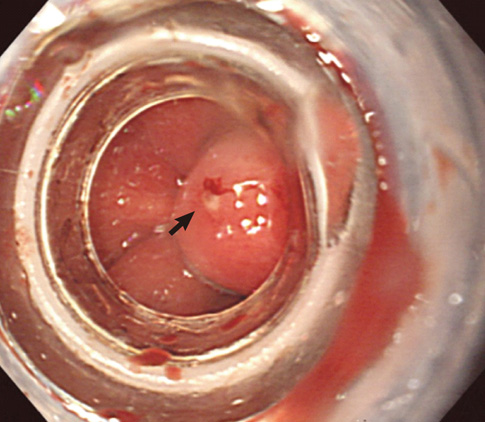
Fig. 1 Endoscopic view showing the ligated gastric varix. This finding indicates successful ligation of the gastric varix at its bleeding site.

Fig. 2 Endoscopic finding and computed tomographic (CT) image, 2 days after the band ligation. (A) Perforation (arrow) was noted by endoscopy at post-EVL ulcer base on the gastric fundus. (B) Abdominal CT image visualized some air bubbles in the posterior aspect of the stomach fundus.
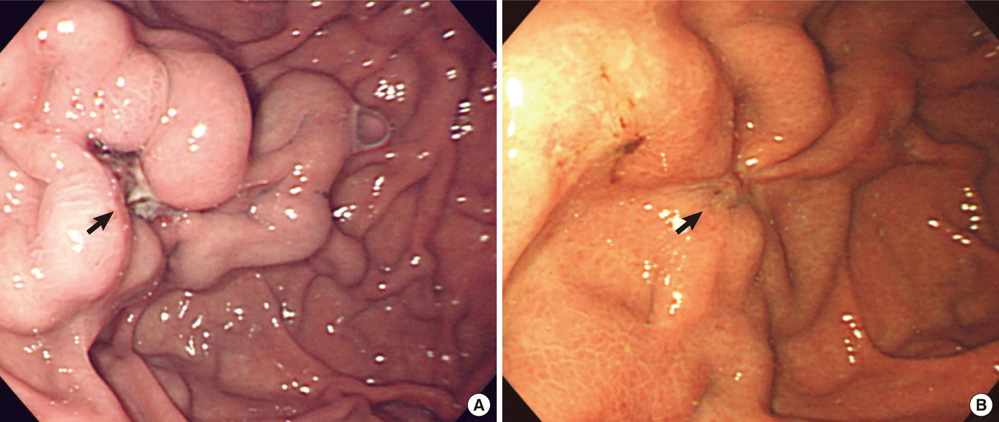
Fig. 3 Follow-up endoscopic findings. (A) Healing ulcer on the perforation site of the gastric fundus 10 days later. (B) Complete remission of the perforated site after 3 months.
Reference
-
1. Kim YS, Um SH, Ryu HS, Lee JB, Lee JW, Park DK, Kim YS, Jin YT, Chun HJ, Lee HS, et al. The prognosis of liver cirrhosis in recent years in Korea. J Korean Med Sci. 2003. 18:833–841.2. De Franchis R, Primignani M. Natural history of portal hypertension in patients with cirrhosis. Clin Liver Dis. 2001. 5:645–663.3. Seo YS, Kim YH, Ahn SH, Yu SK, Baik SK, Choi SK, Heo J, Hahn T, Yoo TW, Cho SH, et al. Clinical features and treatment outcomes of upper gastrointestinal bleeding in patients with cirrhosis. J Korean Med Sci. 2008. 23:635–643.4. Garcia-Tsao G, Sanyal AJ, Grace ND, Carey W. Practice Guidelines Committee of the American Association for the Study of Liver Diseases. Practice Parameters Committee of the American College of Gastroenterology. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007. 46:922–938.5. Sarin SK, Lahoti D, Saxena SP, Murthy NS, Makwana UK. Prevalence, classification and natural history of gastric varices: a long-term follow-up study in 568 portal hypertension patients. Hepatology. 1992. 16:1343–1349.6. Stiegmann GV, Goff JS, Michaletz-Onody PA, Korula J, Lieberman D, Saeed ZA, Reveille RM, Sun JH, Lowenstein SR. Endoscopic sclerotherapy as compared with endoscopic ligation for bleeding esophageal varices. N Engl J Med. 1992. 326:1527–1532.7. Chen WC, Hou MC, Tsay SH, Lo SS, Lin HC, Chang FY, Lee SD. Gastric perforation after endoscopic ligation for gastric varices. Gastrointest Endosc. 2001. 54:99–101.8. Takeuchi M, Nakai Y, Syu A, Okamoto E, Fujimoto J. Endoscopic ligation of gastric varices. Lancet. 1996. 348:1038.9. Matsumoto A, Izumiya T, Takimoto K, Inokuchi H. Management of acute gastric variceal bleeding. Aliment Pharmacol Ther. 2003. 18:1173–1174.10. Suk KT, Baik SK, Yoon JH, Cheong JY, Paik YH, Lee CH, Kim YS, Lee JW, Kim DJ, Cho SW, et al. Revision and update on clinical practice guideline for liver cirrhosis. Korean J Hepatol. 2012. 18:1–21.11. Tan PC, Hou MC, Lin HC, Liu TT, Lee FY, Chang FY, Lee SD. A randomized trial of endoscopic treatment of acute gastric variceal hemorrhage: N-butyl-2-cyanoacrylate injection versus band ligation. Hepatology. 2006. 43:690–697.12. Leung Ki EL, Lau JY. New endoscopic hemostasis methods. Clin Endosc. 2012. 45:224–229.13. Hashiba K, Carvalho AM, Diniz G Jr, Barbosa de Aridrade N, Guedes CA, Siqueira Filho L, Lima CA, Coehlo HE, de Oliveira RA. Experimental endoscopic repair of gastric perforations with an omental patch and clips. Gastrointest Endosc. 2001. 54:500–504.14. Tsibouris P, Zintzaras E, Lappas C, Moussia M, Tsianos G, Galeas T, Potamianos S. High-dose pantoprazole continuous infusion is superior to somatostatin after endoscopic hemostasis in patients with peptic ulcer bleeding. Am J Gastroenterol. 2007. 102:1192–1199.15. Schmassmann A, Reubi JC. Cholecystokinin-B/gastrin receptors enhance wound healing in the rat gastric mucosa. J Clin Invest. 2000. 106:1021–1029.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Esophageal Perforation during Endoscopic Variceal Ligation
- Results of Experimental Canine Gastric Wall Ligation using 0-shaped Rubber Band
- The Influence of EIS or EVL to Gastric Varices in Bleeding Esophageal Varices
- Practical Approach to Endoscopic Management for Bleeding Gastric Varices
- Endoscopic Ligation of Large Gastric Varices Using a Detachable Snares and Rubber Bands
