Parent-Controlled Analgesia in Children Undergoing Cleft Palate Repair
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, and Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Seoul, Korea. ktmin501@yumc.yonsei.ac.kr
- 2Department of Anesthesiology and Pain Medicine, Kwandong University College of Medicine, Goyang, Korea.
- 3Department of Plastic and Reconstructive Surgery, Institute for Human Tissue Restoration, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1786857
- DOI: http://doi.org/10.3346/jkms.2008.23.1.122
Abstract
- The aims of this study were to find an optimal basal infusion dose of fentanyl for parent-controlled analgesia (PrCA) in children undergoing cleft palate repair and the degree of parents' satisfaction with PrCA. Thirty consecutive children between 6 months and 2 yr of age were enrolled. At the end of surgery, a PrCA device with a basal infusion rate of 2 mL/hr and bolus of 0.5 mL with lockout time of 15 min was applied. Parents were educated in patient-controlled analgesia (PCA) devices, the Wong Baker face pain scoring system, and monitoring of adverse effects of fentanyl. Fentanyl was infused 0.3 microgram/kg/hr at first, and we obtained a predetermined fentanyl regimen by the response of the previous patient to a larger or smaller dose of fentanyl (0.1 microgram/kg/hr as the step size), using an up-and-down method. ED50 and ED95 by probit analysis were 0.63 microgram/kg/hr (95% confidence limits, 0.55-0.73 microgram/kg/hr) and 0.83 microgram/kg/hr (95% confidence limits, 0.73-1.47 microgram/kg/hr), respectively. Eighty seven percent of the parents were satisfied with participating in the PrCA modality. PrCA using fentanyl with a basal infusion rate of 0.63 microgram/kg/hr can be applied effectively for postoperative pain management in children undergoing cleft palate repair with a high level of parents' satisfaction.
MeSH Terms
Figure
-
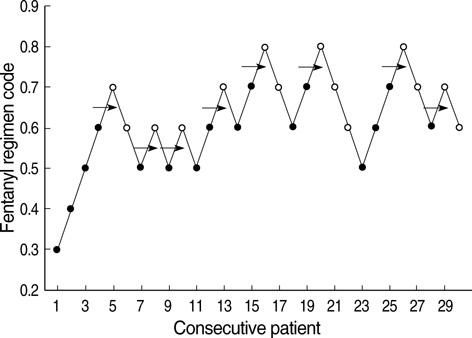
Fig. 1 The responses of 30 consecutive patients by the parent-controlled analgesic (PrCA) modality with different fentanyl regimens. Patient's response to the PrCA regimen was described as 'Effective' (open circle) or 'Not effective' (close circle). Fentanyl regimen was coded by the numeric of the basal infusion rate ( µg/kg/hr). Arrows indicate the midpoint of fentanyl regimens of all independent pairs of patients, involving a crossover from 'Not effective' to 'Effective'.
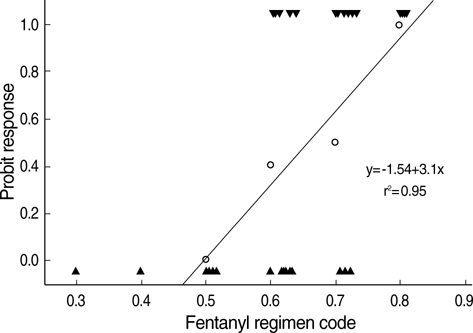
Fig. 2 Probit analysis of fentanyl regimen. Triangles in the bottom represent the patients of 'Not effective', and reverse triangles in the top represent the patients of 'Effective'. Regression plot and line were displayed according to probit analysis.
Cited by 1 articles
-
Small dose of propofol combined with dexamethasone for postoperative vomiting in pediatric Moyamoya disease patients: a prospective, observer-blinded, randomized controlled study
Jeongmin Kim, Gyu Dong Jang, Dong-Suk Kim, Kyeong Tae Min
Korean J Anesthesiol. 2013;64(2):127-132. doi: 10.4097/kjae.2013.64.2.127.
Reference
-
1. Munro HM, Malviya S, Lauder GR, Voepel-Lewis T, Tait AR. Pain relief in children following outpatient surgery. J Clin Anesth. 1999. 11:187–191.
Article2. Peters JW, Bandell Hoekstra IE, Huijer Abu-Saad H, Bouwmeester J, Meursing AE, Tibboel D. Patient controlled analgesia in children and adolescents: a randomized controlled trial. Paediatr Anaesth. 1999. 9:235–241.
Article3. Verghese ST, Hannallah RS. Postoperative pain management in children. Anesthesiol Clin North America. 2005. 23:163–184.
Article4. Kanagasundaram SA, Cooper MG, Lane LJ. Nurse-controlled analgesia using a patient-controlled analgesia device: an alternative strategy in the management of severe cancer pain in children. J Paediatr Child Health. 1997. 33:352–355.
Article5. Roulleau P, Gall O, Desjeux L, Dagher C, Murat I. Remifentanil infusion for cleft palate surgery in young infants. Paediatr Anaesth. 2003. 13:701–707.
Article6. Kehlet H. Procedure-specific postoperative pain management. Anesthesiol Clin North America. 2005. 23:203–210.
Article7. Dell'Oste C, Savron F, Pelizzo G, Sarti A. Acute airway obstruction in an infant with Pierre Robin syndrome after palatoplasty. Acta Anaesthesiol Scand. 2004. 48:787–789.8. Dixon WJ. Staircase bioassay: the up-and-down method. Neurosci Biobehav Rev. 1991. 15:47–50.
Article9. Wong DL, Baker CM. Pain in children: comparison of assessment scales. Pediatr Nurs. 1988. 14:9–17.10. Klimscha W, Chiari A, Michalek-Sauberer A, Wildling E, Lerche A, Lorber C, Brinkmann H, Semsroth M. The efficacy and safety of a clonidine/bupivacaine combination in caudal blockade for pediatric hernia repair. Anesth Analg. 1998. 86:54–61.
Article11. Buttner W, Finke W. Analysis of behavioural and physiological parameters for the assessment of postoperative analgesic demand in newborns, infants and young children: a comprehensive report on seven consecutive studies. Paediatr Anaesth. 2000. 10:303–318.12. Monitto CL, Greenberg RS, Kost-Byerly S, Wetzel R, Billett C, Lebet RM, Yaster M. The safety and efficacy of parent-/nurse-controlled analgesia in patients less than six years of age. Anesth Analg. 2000. 91:573–579.
Article13. Katz R, Kelly HW. Pharmacokinetics of continuous infusions of fentanyl in critically ill children. Crit Care Med. 1993. 21:995–1000.
Article14. Yildiz K, Tercan E, Dogru K, Ozkan U, Boyaci A. Comparison of patient-controlled analgesia with and without a background infusion after appendicectomy in children. Paediatr Anaesth. 2003. 13:427–431.
Article15. Kelly AM, Powell CV, Williams A. Parent visual analogue scale ratings of children's pain do not reliably reflect pain reported by child. Pediatr Emerg Care. 2002. 18:159–162.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparative study of levobupivacaine and bupivacaine for bilateral maxillary nerve block during pediatric primary cleft palate surgery: a randomized double-blind controlled study
- Dexmedetomidine during suprazygomatic maxillary nerve block for pediatric cleft palate repair, randomized double-blind controlled study
- A novel modification of Bardach’s two-flap palatoplasty for the repair of a difficult cleft palate
- Cause analysis, prevention, and treatment of postoperative restlessness after general anesthesia in children with cleft palate
- Clinical Experience of Cleft Lip and/or Palate Repair in Complex Congenital Heart Disease
