J Korean Med Sci.
2014 May;29(5):685-690. 10.3346/jkms.2014.29.5.685.
The Relationship Between J Wave on the Surface Electrocardiography and Ventricular Fibrillation during Acute Myocardial Infarction
- Affiliations
-
- 1Department of Internal Medicine, Inha University Hospital, Incheon, Korea. kdhmd@inha.ac.kr
- KMID: 1786111
- DOI: http://doi.org/10.3346/jkms.2014.29.5.685
Abstract
- We investigated whether the presence of J wave on the surface electrocardiography (sECG) could be a potential risk factor for ventricular fibrillation (VF) during acute myocardial infarction (AMI). We performed a retrospective study of 317 patients diagnosed with AMI in a single center from 2009 to 2012. Among the enrolled 296 patients, 22 (13.5%) patients were selected as a VF group. The J wave on the sECG was defined as a J point elevation manifested through QRS notching or slurring at least 1 mm above the baseline in at least two leads. We found that the incidence of J wave on the sECG was significantly higher in the VF group. We also confirmed that several conventional risk factors of VF were significantly related to VF during AMI; time delays from the onset of chest pain, blood concentrations of creatine phosphokinase and incidence of ST-segment elevation. Multiple logistic regression analysis demonstrated that the presence of J wave and the presence of a ST-segment elevation were independent predictors of VF during AMI. This study demonstrated that the presence of J wave on the sECG is significantly related to VF during AMI.
MeSH Terms
Figure
-
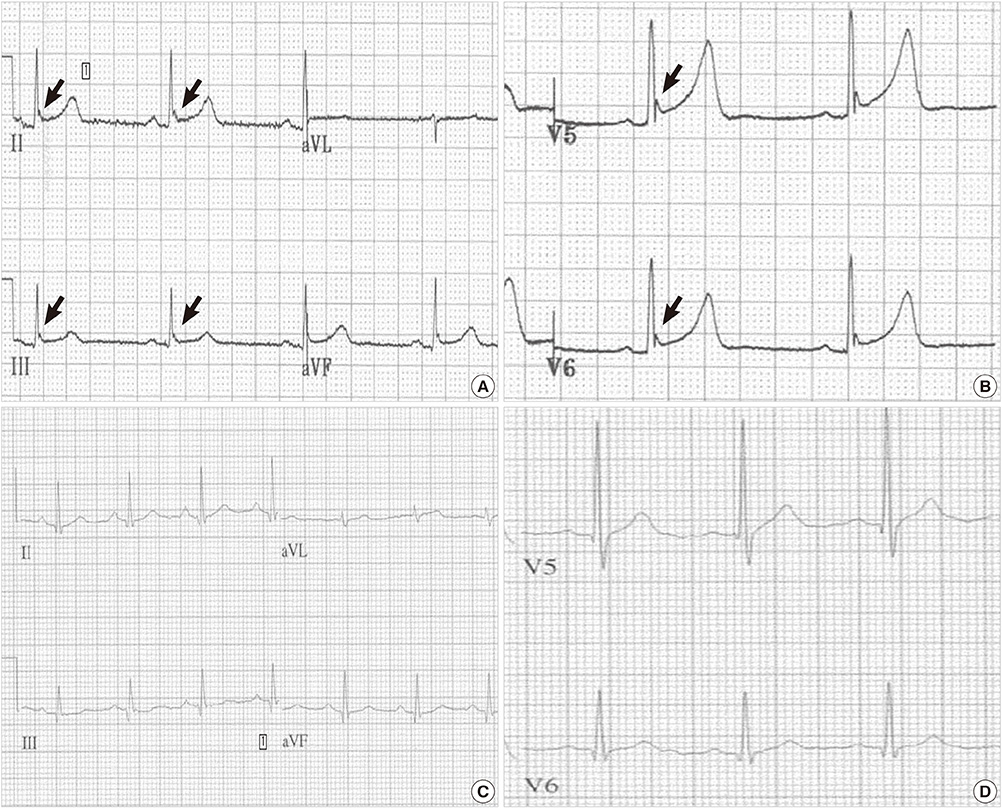
Fig. 1 Baseline ECGs in AMI patients. (A) and (B) show notched elevations (arrows) in inferior (A) and lateral (B) leads in the patients who had an event of VF, whereas (C) and (D). show no J wave in inferior (C) or lateral (D) leads in the patients who showed no VF during AMI.
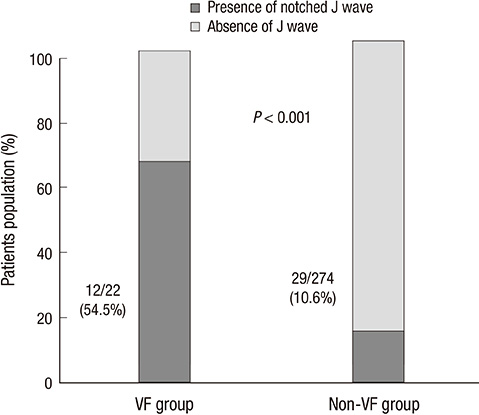
Fig. 2 Relationship between notched J wave and VF.The incidence of J wave is significantly higher in the VF group.
Reference
-
1. Gheeraert PJ, De Buyzere ML, Taeymans YM, Gillebert TC, Henriques JP, De Backer G, De Bacquer D. Risk factors for primary ventricular fibrillation during acute myocardial infarction: a systematic review and meta-analysis. Eur Heart J. 2006; 27:2499–2510.2. Ogawa M, Kumagai K, Yamanouchi Y, Saku K. Spontaneous onset of ventricular fibrillation in Brugada syndrome with J wave and ST-segment elevation in the inferior leads. Heart Rhythm. 2005; 2:97–99.3. Patel RB, Ng J, Reddy V, Chokshi M, Parikh K, Subacius H, Alsheikh-Ali AA, Nguyen T, Link MS, Goldberger JJ, et al. Early repolarization associated with ventricular arrhythmias in patients with chronic coronary artery disease. Circ Arrhythm Electrophysiol. 2010; 3:489–495.4. Naruse Y, Tada H, Harimura Y, Hayashi M, Noguchi Y, Sato A, Yoshida K, Sekiguchi Y, Aonuma K. Early repolarization is an independent predictor of occurrences of ventricular fibrillation in the very early phase of acute myocardial infarction. Circ Arrhythm Electrophysiol. 2012; 5:506–513.5. Rudic B, Veltmann C, Kuntz E, Behnes M, Elmas E, Konrad T, Kuschyk J, Weiss C, Borggrefe M, Schimpf R. Early repolarization pattern is associated with ventricular fibrillation in patients with acute myocardial infarction. Heart Rhythm. 2012; 9:1295–1300.6. Aizawa Y, Jastrzebski M, Ozawa T, Kawecka-Jaszcz K, Kukla P, Mitsuma W, Chinushi M, Ida T, Aizawa Y, Ojima K, et al. Characteristics of electrocardiographic repolarization in acute myocardial infarction complicated by ventricular fibrillation. J Electrocardiol. 2012; 45:252–259.7. Gussak I, Antzelevitch C. Early repolarization syndrome: clinical characteristics and possible cellular and ionic mechanisms. J Electrocardiol. 2000; 33:299–309.8. Haïssaguerre M, Derval N, Sacher F, Jesel L, Deisenhofer I, de Roy L, Pasquié JL, Nogami A, Babuty D, Yli-Mayry S, et al. Sudden cardiac arrest associated with early repolarization. N Engl J Med. 2008; 358:2016–2023.9. Rosso R, Kogan E, Belhassen B, Rozovski U, Scheinman MM, Zeltser D, Halkin A, Steinvil A, Heller K, Glikson M, et al. J-point elevation in survivors of primary ventricular fibrillation and matched control subjects: incidence and clinical significance. J Am Coll Cardiol. 2008; 52:1231–1238.10. Antzelevitch C. Genetic, molecular and cellular mechanisms underlying the J wave syndromes. Circ J. 2012; 76:1054–1065.11. Miyazaki S, Shah AJ, Haïssaguerre M. Early repolarization syndrome - a new electrical disorder associated with sudden cardiac death. Circ J. 2010; 74:2039–2044.12. Miyazaki T, Mitamura H, Miyoshi S, Soejima K, Aizawa Y, Ogawa S. Autonomic and antiarrhythmic drug modulation of ST segment elevation in patients with Brugada syndrome. J Am Coll Cardiol. 1996; 27:1061–1070.13. Yan GX, Joshi A, Guo D, Hlaing T, Martin J, Xu X, Kowey PR. Phase 2 reentry as a trigger to initiate ventricular fibrillation during early acute myocardial ischemia. Circulation. 2004; 110:1036–1041.14. Volders PG, Sipido KR, Carmeliet E, Spätjens RL, Wellens HJ, Vos MA. Repolarizing K+ currents ITO1 and IKs are larger in right than left canine ventricular midmyocardium. Circulation. 1999; 99:206–210.15. Tikkanen JT, Junttila MJ, Anttonen O, Aro AL, Luttinen S, Kerola T, Sager SJ, Rissanen HA, Myerburg RJ, Reunanen A, et al. Early repolarization: electrocardiographic phenotypes associated with favorable long-term outcome. Circulation. 2011; 123:2666–2673.16. Rosso R, Adler A, Halkin A, Viskin S. Risk of sudden death among young individuals with J waves and early repolarization: putting the evidence into perspective. Heart Rhythm. 2011; 8:923–929.17. Volpi A, Cavalli A, Santoro L, Negri E. Incidence and prognosis of early primary ventricular fibrillation in acute myocardial infarction: results of the Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto Miocardico (GISSI-2) database. Am J Cardiol. 1998; 82:265–271.18. Bezzina CR, Pazoki R, Bardai A, Marsman RF, de Jong JS, Blom MT, Scicluna BP, Jukema JW, Bindraban NR, Lichtner P, et al. Genome-wide association study identifies a susceptibility locus at 21q21 for ventricular fibrillation in acute myocardial infarction. Nat Genet. 2010; 42:688–691.19. Haïssaguerre M, Chatel S, Sacher F, Weerasooriya R, Probst V, Loussouarn G, Horlitz M, Liersch R, Schulze-Bahr E, Wilde A, et al. Ventricular fibrillation with prominent early repolarization associated with a rare variant of KCNJ8/KATP channel. J Cardiovasc Electrophysiol. 2009; 20:93–98.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dispersion of QT Interval and Other Repolarization Indexes in Acute Myocardial Infarction
- Clinical Feature of Non-Q Wave Myocardial infarction : Relationship with EKG Findings and Infarct Related Arteries
- Aconitine Intoxication Misdiagnosed as Acute Myocardial Infarction
- Correlation between Abnormal Q Wave in Leads I or aVL and First Diagonal Branch Stenosis in Patients with Acute Myocardial Infarction
- Case of Recurrent Ventricular Fibrillations with Osborn Wave Developed during Therapeutic Hypothermia
