J Korean Med Sci.
2008 Aug;23(4):723-726. 10.3346/jkms.2008.23.4.723.
A Case of Kawasaki Disease with Colonic Edema
- Affiliations
-
- 1Department of Pediatrics, Soonchunhyang University Hospital, Gumi, Korea. ped0921@hanmail.net
- KMID: 1785837
- DOI: http://doi.org/10.3346/jkms.2008.23.4.723
Abstract
- Kawasaki disease (KD) is recognized as a systemic vasculitis affecting multi-organ with inflammatory changes. The commonest and most serious complication of KD is coronary artery aneurysm, but KD may cause other organic complications beside cardiac problems. Gastrointestinal tract also present complications of KD in which, for example, hepatic dysfunction, pancreatitis, intussusception, colonic obstruction, intestinal pseudo-obstruction, and bowel edema are included. Among them, colonal wall edema is left unknown in the incidence, and it has been reported even if rare. In this report, we describe a case of KD with colonal wall edema, occurred in 5-yr-old boy who complained of severe abdominal pain and vomiting.
MeSH Terms
Figure
-

Fig. 1 Abdominal radiograph reveals distended bowel loop with fecal materials.
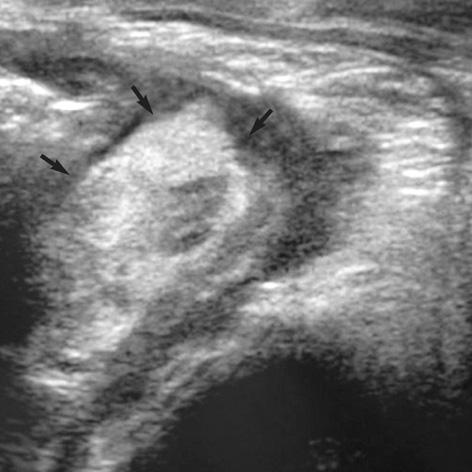
Fig. 2 Transabdominal ultrasonograph shows circumferential bowel wall thickening (arrows) in the descending and sigmoid colon.

Fig. 3 (A) Contrast-enhanced abdominal CT reveals circumferential bowel wall thickening with submucosal low attenuation in the lower distal descending colon (arrows). There are no abnormal enhanced lesion in pelvic solid organs and no ascites in the pelvic cavity. (B) Abdominal CT reveals circumferential bowel wall thickening in the sigmoid colon (black arrows), but normal thickness in the rectum (white arrows).
Reference
-
1. Kawasaki T. Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children. Arerugi. 1967. 16:178–222.2. Chung CJ, Stein L. Kawasaki disease: a review. Radiology. 1998. 208:25–33.
Article3. Tizard EJ. Complication of Kawasaki disease. Current Paediatrics. 2005. 15:62–68.4. Yaniv L, Jaffe M, Shaoul R. The surgical manifestations of the intestinal tract in Kawasaki disease. J Pediatr Surg. 2005. 40:e1–e4.
Article5. Miyake T, Kawamori J, Yoshida T, Nakano H, Kohno S, Ohba S. Small bowel pseudo-obstruction in Kawasaki disease. Pediatr Radiol. 1987. 17:383–386.
Article6. Burgner D, Harnden A. Kawasaki disease: What is the epidemiology telling us about the etiology? Int J Infect Dis. 2005. 9:185–194.
Article7. Cimaz R, Falcini F. An update on Kawasaki disease. Autoimmun Rev. 2003. 2:258–263.
Article8. Tizard EJ, Suzuki A, Levin M, Dillon MJ. Clinical aspects of 100 patients with Kawasaki disease. Arch Dis Child. 1991. 66:185–188.
Article9. Zulian F, Falcini F, Zancan L, Martini G, Secchieri S, Luzzatto C, Zacchello F. Acute surgical abdomen as presenting manifestation of Kawasaki disease. J Pediatr. 2003. 142:731–735.
Article10. Murphy DJ Jr, Morrow WR, Harberg FJ, Hawkins EP. Small bowel obstruction as a complication of Kawasaki disease. Clin Pediatr (Phila). 1987. 26:193–196.
Article11. Fan ST, Lau WY, Wong KK. Ischemic colitis in Kawasaki disease. J Pediatr Surg. 1986. 21:964–965.
Article12. Yamashiro Y, Nagata S, Ohtsuka Y, Oguchi S, Shimizu T. Microbiologic studies on the small intestine in Kawasaki disease. Pediatr Res. 1996. 39:622–624.
Article
