The Value of Initial Ionized Calcium as a Predictor of Mortality and Triage Tool in Adult Trauma Patients
- Affiliations
-
- 1Department of Surgery, Masan Samsung Hospital, Sungkyunkwan University School of Medicine, Masan, Korea.
- 2Department of Emergency Medicine, Masan Samsung Hospital, Sungkyunkwan University School of Medicine, Masan, Korea. syellow@paran.com
- KMID: 1785832
- DOI: http://doi.org/10.3346/jkms.2008.23.4.700
Abstract
- Ionized hypocalcemia is a common finding in critically ill patients, but the relationship between ionized hypocalcemia and mortality risk in trauma patients has not been well established. The aim of this study was to assess the usefulness of initial ionized calcium (iCa) in predicting mortality in the trauma population, and evaluate its superiority over the three other triage tools: base deficit, systemic inflammatory response syndrome (SIRS) score, and triage-revised trauma score (t-RTS). A proand retrospective study was performed on 255 consecutive trauma patients admitted to our Emergency Medical Center from January to December, 2005, who underwent arterial blood gas analysis. Multivariate logistic regression analysis confirmed iCa (< or =0.88 mM/L), low Glasgow coma scale score, and a large transfusion amount to be significant risk factors associated with mortality (p<0.05). The sensitivities of iCa, base deficit, SIRS score, and t-RTS were 82.9%, 76.4%, 67.1%, and 74.5%, and their specificities were 41.0%, 64.1%, 64.1%, and 87.2%, respectively. Receiver operating characteristic curve analysis determined the areas under the curves of these parameters to be 0.607+/-0.062, 0.736+/-0.056, 0.694+/-0.059, and 0.875 +/-0.043, respectively (95% confidence interval). Although initial iCa (< or =0.88 mM/L) was confirmed as a significant risk factor associated with mortality, it exhibited a poorer discriminative power for mortality prediction than other predictors, especially t-RTS.
Keyword
MeSH Terms
Figure
-
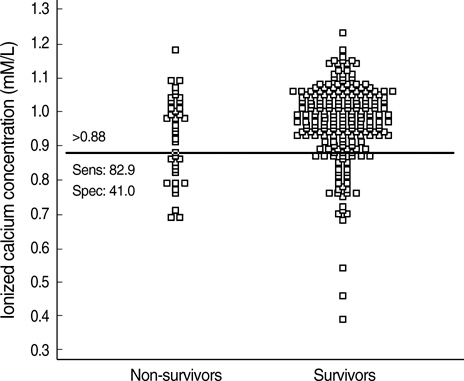
Fig. 1 Interactive dot diagram of trauma patients relative to ionized calcium levels. The horizontal line indicates the cut-off point with the best separation (minimized false negative and false positive results) between the two groups. The cut-off point of ionized calcium level was 0.88 mM/L. The corresponding test characteristics of sensitivity and specificity were 82.9% and 41.0%, respectively.

Fig. 2 The receiver operating characteristic curves of ionized calcium, base deficit, systemic inflammatory response syndrome (SIRS) score, and triage-revised trauma score (t-RTS) in predicting mortality. The areas under the curves (AUC) of these indicators were 0.607±0.062, 0.736±0.056, 0.694±0.059, and 0.875±0.043, respectively (95% confidence interval). The AUC of iCa was not different from that of SIRS, but smaller than those of the other predictors (p<0.05). The AUC of t-RTS was the largest (p<0.01).
Reference
-
1. Drop LJ. Ionized calcium, the heart, and hemodynamic function. Anesth Analg. 1985. 64:432–451.
Article2. Power ML, Heaney RP, Kalkwarf HJ, Pitkin RM, Repke JT, Tsang RC, Schulkin J. The role of calcium in health and disease. Am J Obstet Gynecol. 1999. 181:1560–1569.
Article3. Rasmussen H. The calcium messenger system. N Engl J Med. 1986. 314:1094–1101. 1164–1170.
Article4. Zaloga GP. Hypocalcemia in critically ill patients. Crit Care Med. 1992. 20:251–262.
Article5. Bushinsky DA, Monk RD. Electrolyte quintet: calcium. Lancet. 1998. 352:306–311.6. Zivin JR, Gooley T, Zager RA, Ryan MJ. Hypocalcemia: a pervasive metabolic abnormality in the critically ill. Am J Kidney Dis. 2001. 37:689–698.
Article7. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992. 101:1644–1655.8. Champion HR, Sacco WJ, Copes WS, Gann DS, Gennarelli TA, Flanagan ME. A revision of the trauma score. J Trauma. 1989. 29:623–629.
Article9. Fulgenico JP, Riou B, Devilliers C, Guesde R, Saada M, Viars P. Plasma ionized calcium in brain-dead patients. Intensive Care Med. 1995. 21:832–837.
Article10. Vivien B, Langeron O, Morell E, Devilliers C, Carli PA, Coriat P, Riou B. Early hypocalcemia in severe trauma. Crit Care Med. 2005. 33:1946–1952.
Article11. Denlinger JK, Nahrwold ML, Gibbs PS, Lecky JH. Hypocalcaemia during rapid blood transfusion in anaesthetized man. Br J Anaesth. 1976. 48:995–1000.
Article12. Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983. 148:839–843.
Article13. Carlstedt F, Lind L, Rastad J, Stjernstrom H, Wide L, Ljunghall S. Parathyroid hormone and ionized calcium levels are related to the severity of illness and survival in critically ill patients. Eur J Clin Invest. 1998. 28:898–903.
Article14. Burchard KW, Gann DS, Colliton J, Forster J. Ionized calcium, parathormone, and mortality in critically ill surgical patients. Ann Surg. 1990. 212:543–549.15. Forman DT, Lorenzo L. Ionized calcium: its significance and clinical usefulness. Ann Clin Lab Sci. 1991. 21:297–304.16. Vincent JL, Bredas P, Jankowski S, Kahn RJ. Correction of hypocalcaemia in the critically ill: what is the haemodynamic benefit? Intensive Care Med. 1995. 21:838–841.
Article17. Hurley K, Baggs D. Hypocalcemic cardiac failure in the emergency department. J Emerg Med. 2005. 28:155–159.
Article18. James MF, Roche AM. Dose-response relationship between plasma ionized calcium concentration and thrombelastography. J Cardiothorac Vasc Anesth. 2004. 18:581–586.
Article19. Hastbacka J, Pettila V. Prevalence and predictive value of ionized hypocalcemia among critically ill patients. Acta Anaesthesiol Scand. 2003. 47:1264–1269.
Article20. Cherry RA, Bradburn E, Carney DE, Shaffer ML, Gabbay RA, Cooney RN. Do early ionized calcium levels really matter in trauma patients? J Trauma. 2006. 61:774–779.
Article21. Randolph AG, Guyatt GH, Calvin JE, Doig G, Richardson WS. Understanding articles describing clinical prediction tools. Crit Care Med. 1998. 26:1603–1612.
Article22. Ruttimann UE. Statistical approaches to development and validation of predictive instruments. Crit Care Clin. 1994. 10:19–35.
Article23. Lee EH, Choi JY, Choi YC, Hwang SY. The usefulness of initial arterial base deficit in trauma patients. J Korean Soc Traumatol. 2006. 19:67–73.24. Gill MR, Reiley DG, Green SM. Interrater reliability of Glasgow coma scale scores in the emergency department. Ann Emerg Med. 2004. 43:215–223.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relationship between Direct Measured and Calculated Ionized Calcium in Maintenance Hemodialysis Patients
- Frequency of Serum Ionized Hypomagnesemia in Patient with Ionized Hypocalcemia
- The Effects of Lithium Treatment on the Serum Calcium, Ionized Calcium & Phosphate in Bipolar Disorder
- Whole blood versus serum ionized calcium concentrations in dialysis patients
- Mortality and Morbidity in Severely Traumatized Elderly Patients
