Limited Feasibility in Endovascular Aneurysm Repair Using Currently Available Graft in Korea
- Affiliations
-
- 1Department of Surgery, Seoul National University Bundang Hospital, Seongnam, Korea. tslee@snubh.org
- 2Department of Surgery, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 1785824
- DOI: http://doi.org/10.3346/jkms.2008.23.4.651
Abstract
- Despite the wide acceptance of endovascular aneurysmal repair in patients with abdominal aortic aneurysm (EVAR), stringent morphologic criteria recommended by manufacturers may preclude this treatment in patients with AAA. The purpose of this study was to investigate how many patients are feasible by Zenith and Excluder stent graft system, which are available in Korea. Eighty-two AAA patients (71 men, mean age 70 yr) who had been treated surgically or medically from January 2005 to December 2006 were included. Criteria for morphologic suitability (MS) were examined to focus on characteristics of aneurysm; proximal and distal landing zone; angulation and involvement of both iliac artery aneurysms. Twenty-eight patients (34.1%) were feasible in Zenith stent graft and 31 patients (37.8%) were feasible in Excluder. The patients who were excluded EVAR had an average of 1.61 exclusion criteria. The main reasons for exclusion were an unfavorable proximal neck (n=34, 41.5%) and problem of distal landing zone (n=25, 30.5%). There was no statistical significance among gender, age or aneurysm size in terms of MS. Only 32 patients (39%) who had AAA were estimated to be suitable for two currently approved grafts by strict criteria. However, even unfavorable AAA patients who have severe co-mobidities will be included in EVAR in the near future. Therefore, more efforts including fine skill and anatomical understanding will be needed to meet these challenging cases.
Keyword
MeSH Terms
Figure
-
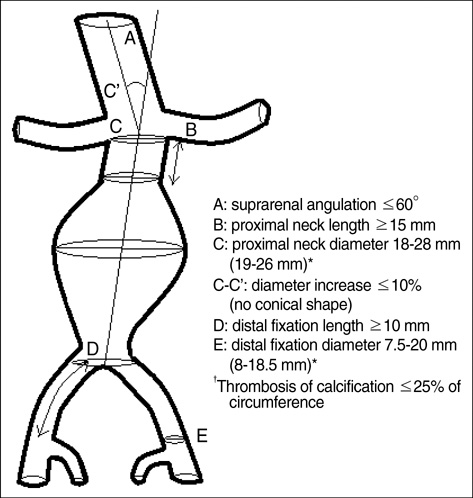
Fig. 1 Schematic review of Zenith inclusion criteria. *, inclusion criteria of Excluder, 2006.
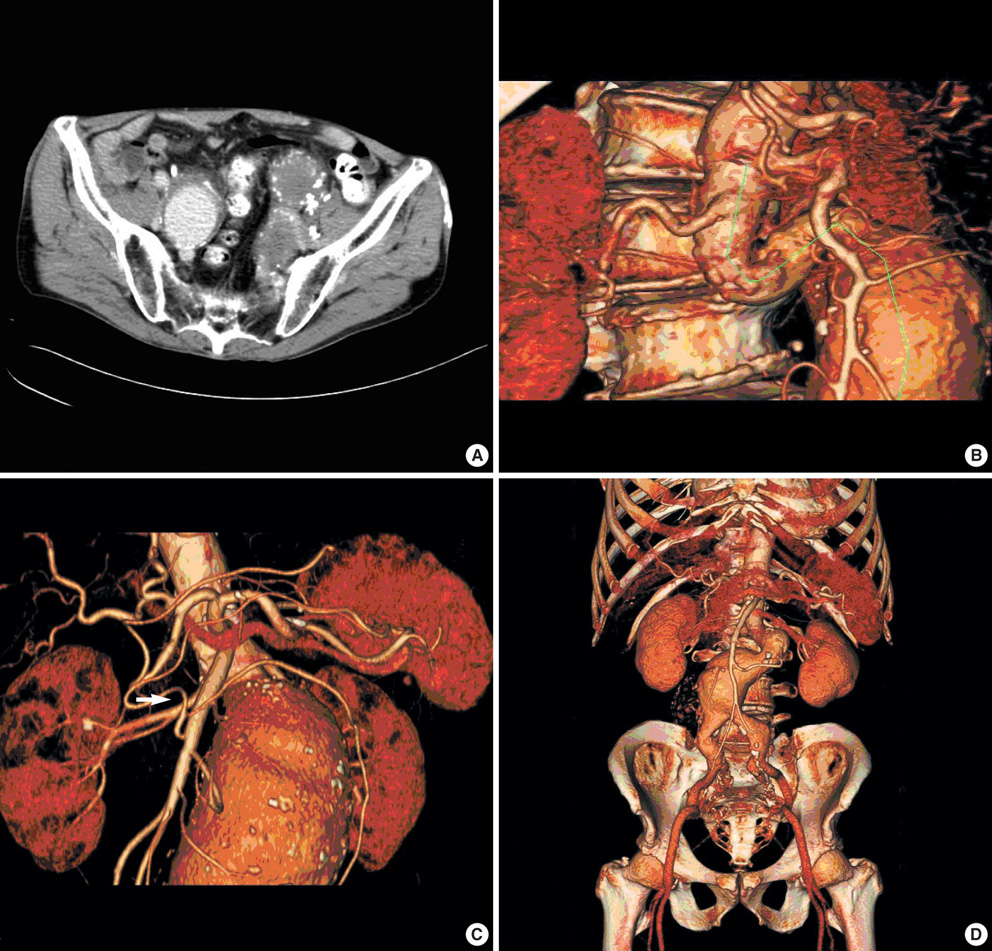
Fig. 2 Cases that were excluded for EVAR (A) CIA aneurysm involving both EIA and IIA. No feasible distal fixation zone was shown. (B) Inadequate infrarenal angle (125.9°). (C) Proximal short neck. Arrow indicates the lowest renal artery. The distance from lower margin of renal artery to aneurysm neck is about 5 mm. (D) Bilateral CIA aneurysm. Both CIA diameter was measured over 20 mm at the iliac bifurcation level.
Cited by 1 articles
-
Outcomes after Elective Open Abdominal Aortic Aneurysm Repair in Octogenarians Compared to Younger Patients in Korea
Joon-Kee Park, Jihee Kang, Young-Wook Kim, Dong-Ik Kim, Seon-Hee Heo, Eunmi Gil, Shin-Young Woo, Yang-Jin Park
J Korean Med Sci. 2021;36(47):e314. doi: 10.3346/jkms.2021.36.e314.
Reference
-
1. Parodi JC, Palmaz JC, Barone HD. Transfemoral intraluminal graft implantation for abdominal aortic aneurysms. Ann Vasc Surg. 1991. 5:491–499.
Article2. Rockman C. Reducing complications by better case selection: anatomic considerations. Semin Vasc Surg. 2004. 17:298–306.
Article3. Masuda EM, Caps MT, Singh N, Yorita K, Schneider PA, Sato DT, Eklof B, Nelken NA, Kistner RL. Effect of ethnicity on access and device complications during endovascular aneurysm repair. J Vasc Surg. 2004. 40:24–29.
Article4. Greenhalgh RM, Brown LC, Kwong GP, Powell JT, Thompson SG. EVAR trial participants. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: randomized controlled trial. Lancet. 2004. 364:843–848.5. EVAR trial participants. Endovascular aneurysm repair versus open repair in patients with abdominal aortic aneurysm (EVAR trial 1): randomized controlled trial. Lancet. 2005. 365:2179–2186.6. Prinssen M, Verhoeven EL, Buth J, Cuypers PW, Van Sambeek MR, Balm R, Buskens E, Grobbee DE, Blankensteijn JD; Dutch Randomized Endovascular Aneurysm Management (DREAM) Trial Group. A randomized trial comparing conventional and endovascular repair of abdominal aortic aneurysms. N Engl J Med. 2004. 351:1607–1618.
Article7. Drury D, Michaels JA, Jones L, Ayiku L. Systematic review of recent evidence for the safety and efficacy of elective endovascular repair in the management of infrarenal abdominal aortic aneurysm. Br J Surg. 2005. 92:937–946.
Article8. Vogel TR, Nackman GB, Crowley JG, Bueno MM, Banavage A, Odroniec K, Brevetti LS, Ciocca RG, Graham AM. Factors impacting functional health and resource utilization following abdominal aortic aneurysm repair by open and endovascular techniques. Ann Vasc Surg. 2005. 19:641–647.
Article9. Brewster DC, Jones JE, Chung TK, Lamuraglia GM, Kwolek CJ, Watkins MT, Hodgman TM, Cambria RP. Long-term outcomes after Endovascular abdominal aortic aneurysm repair. The first decade. Ann Surg. 2006. 244:426–438.10. Kim YW, Min SK, Koh YB, Kim SN, Park JS, Moon IS, Park SW, Huh S, Choi JY, Park H, Cho WH, Kim HT, Park KH, Rhee JA, Cho KJ, Chung SW, Kim YS, Kim DI, Do YS, Kim SJ, Ha J, Park JH, Ahn H, Lee T, Choh JH, Kim D, Shim WH, Lee DY, Kwun KB, Suh BY, Kwun WH, Cho YP, Kim GE, Kwon TW, Cho HR, So BJ, Jun HJ, Kim SK, Chung SY, Choi SJ, Kim SH, Chang JH, Jang LC, Kim IG, Kim HC. Report of nation-wide Questionnaire survey for abdominal aortic aneurysm treatment in Korea. J Korean Vasc Surg. 2005. 21:10–15.11. Elkouri S, Martelli E, Gloviczki P, McKusick MA, Panneton JM, Andrews JC, Noel AA, Bower TC, Sullivan TM, Rowland C, Hoskin TL, Cherry KJ. Most patients with abdominal aortic aneurysm are not suitable for endovascular repair using currently approved bifurcated stent-grafts. Vasc Endovascular Surg. 2004. 38:401–412.
Article12. Carpenter JP, Baum RA, Barker CF, Golden MA, Mitchell ME, Velazquez OC, Fairman RM. Impact of exclusion criteria on patient selection for endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2001. 34:1050–1054.
Article13. Cotroneo AR, Iezzi R, Giancristofaro D, Santoro M, Quinto F, Spigonardo F, Storto ML. Endovascular abdominal aortic aneurysm repair: how many patients are eligible for endovascular repair? Radiol Med (Torino). 2006. 111:597–606.
Article14. Ouriel K, Tanquilut E, Greenberg RK, Walker E. Aortoiliac morphologic correlations in aneurysms undergoing endovascular repair. J Vasc Surg. 2003. 38:323–328.
Article15. Green RM. Patient selection for endovascular abdominal aortic aneurysm repair. J Am Coll Surg. 2002. 194:Suppl 1. S67–S73.
Article16. Waasdorp EJ, De Vries JP, Hobo R, Leurs LJ, Buth J, Moll FL; EUROSTAR Collborators. Aneurysm diameter and proximal aortic neck diameter influnce clinical outcome of endovascular abdominal aortic repair; a 4-year EUROSTAR experience. Ann Vasc Surg. 2005. 19:755–761.17. Aarts F, Van Sterkenburg S, Blankensteijn JD. Endovascular aneurysm repair versus open aneurysm repair: comparison of treatment outcome and procedure-related reintervention rate. Ann Vasc Surg. 2005. 19:699–704.
Article18. Cheng SW, Ting AC, Ho P, Poon JT. Aortic aneurysm morphology in Asians: features affecting stent-graft application and design. J Endovasc Ther. 2004. 11:605–612.19. Welborn MB, Yau FS, Modrall JG, Lopez JA, Floyd S, Valentine RJ, Clagett GP. Endovascular repair of small abdominal aortic aneurysms: a paradigm shift? Vasc Endovascular Surg. 2005. 39:381–391.
Article20. Greenberg RK, Clair D, Srivastava S, Bhandari G, Turc A, Hampton J, Popa M, Green R, Ouriel K. Should patients with challenging anatomy be offered endovascular aneurysm repair? J Vasc Surg. 2003. 38:990–996.
Article21. Sampaio SM, Panneton JM, Mozes GI, Andrews JC, Bower TC, Karla M, Noel AA, Cherry KJ, Sullivan T, Gloviczki P. Proximal type I endoleak after endovascular abdominal aortic aneurysm repair: predictive factors. Ann Vasc Surg. 2004. 18:621–628.
Article22. Moise MA, Woo EY, Velazquez OC, Fairman RM, Golden MA, Mitchell ME, Carpenter JP. Barriers to endovascular aortic aneurysm repair: past experience and implications for future device development. Vasc Endovascular Surg. 2006. 40:197–203.
Article23. Noel AA. Beyond the instructions for use:pushing the limits of infrarenal device application for abdominal aortic aneurysms. Perspect Vasc Surg Endovasc Ther. 2006. 18:19–23.24. Verhoeven EL, Prins TR, Tielliu IF, van den Dungen JJ, Zeebregts CJ, Hulsebos RG, van Andringa de Kempenaer MG, Oudkerk M, van Schilfgaarde R. Treatment of short-necked infrarenal aortic aneurysm with fenestrated stent-graft: short-term results. Eur J Vasc Endovasc Surg. 2004. 27:477–483.25. Lee WA, Nelson PR, Berceli SA, Seeger JM, Huber TS. Outcome after hypogastric artery bypass and embolization during endovascular aneurysm repair. J Vasc Surg. 2006. 44:1162–1168.
Article26. Unno N, Inuzuka K, Yamamoto N, Sagara D, Suzuki M, Konno H. Preservation of pelvic circulation with hypogastric artery bypass in endovascular repair of abdominal aortic aneurysm with bilateral iliac artery aneurysms. J Vasc Surg. 2006. 44:1170–1175.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Repair of Thoracic Aortic Aneurysm Using a Custom-made Fenestrated Stent Graft to Preserve the Left Subclavian Artery
- Endovascular Treatment of Abdominal Aortic Aneurysm
- Endovascular Repair of a Juxtarenal Abdominal Aortic Aneurysm Using a Chimney Graft
- The Complications and Their Management after Endovascular Aneurysm Repair for the Treatment of Abdominal Aortic Aneurysms
- Endovascular Stent-Graft Placement and Secondary Intervention for Abdominal Aortic Aneurysm in a Patient who had a Previously Inserted Iliac Stent
