Pituitary Apoplexy Complicated by Chemical Meningitis and Cerebral Infarction
- Affiliations
-
- 1Department of Neurosurgery, Kosin University College of Medicine Gospel Hospital, Busan, Korea. cuttage@empal.com
- 2Department of Pathology, Kosin University College of Medicine Gospel Hospital, Busan, Korea.
- KMID: 1785776
- DOI: http://doi.org/10.3346/jkms.2007.22.6.1085
Abstract
- A 41-yr-old man was admitted with acute headache, neck stiffness, and febrile sensation. Cerebrospinal fluid examination showed pleocytosis, an increased protein level and, a decreased glucose concentration. No organisms were observed on a culture study. An imaging study revealed pituitary macroadenoma with hemorrhage. On the 7th day of the attack, confusion, dysarthria, and right-sided facial paralysis and hemiparesis were noted. Cerebral infarction on the left basal ganglia was confirmed. Neurologic deficits gradually improved after removal of the tumor by endoscopic transnasal transsphenoidal approach. It is likely that the pituitary apoplexy, aseptic chemical meningitis, and cerebral infarction are associated with each other. This rare case can serve as a prime example to clarify the chemical characteristics of pituitary apoplexy.
Keyword
MeSH Terms
Figure
-
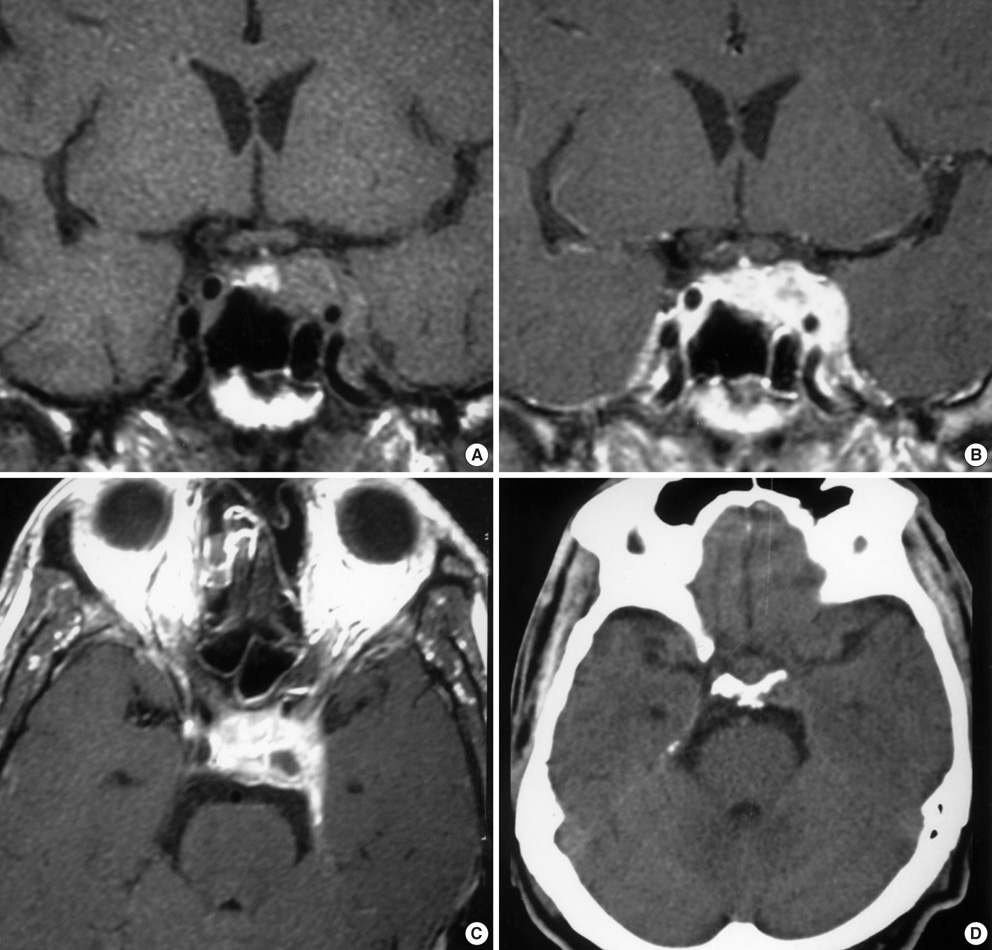
Fig. 1 (A) T1-weighted non-enhanced coronal magnetic resonance imaging (MRI) shows a pituitary mass with increased focal signal intensity that reflects intratumoral hemorrhage. (B) T1-weighted enhanced coronal MRI shows strong enhancement of the pituitary tumor extending to the left cavernous sinus, but not compromising the optic chiasm. (C) Enhanced axial image of MRI shows a high signal intensity lesion and a small cystic area. (D) There is no hemorrhage in the subarachnoid space of the basal cistern on an initial computerized tomography scan.
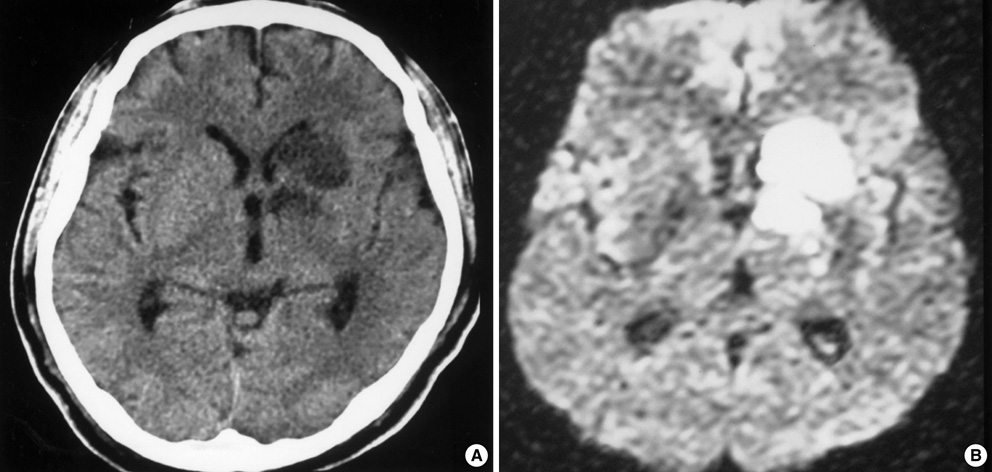
Fig. 2 (A) On the 7th day of pituitary apoplexy, non-contrast computerized tomography scan shows low density on deep nuclei and internal capsule. (B) Diffusion-weighted image of magnetic resonance imaging scan reveals hyperintense infarction in the same area.
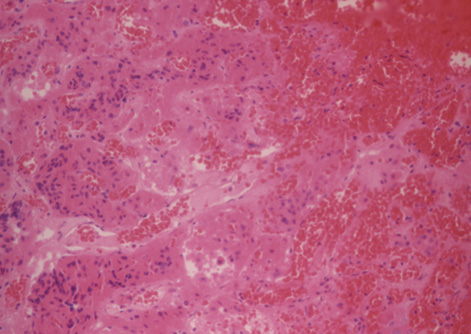
Fig. 3 Histology of pituitary adenoma reveals hemorrhagic infarct with necrotic neoplastic cells and congested vessels supporting the diagnosis of pituitary apoplexy (H&E stain, ×200).
Cited by 1 articles
-
A Case of Unusual Pituitary Apoplexy Presented as Aseptic Meningitis
Kang Min Park, Yeon Mee Kim, Si Eun Kim, Kyong Jin Shin, Sam Yeol Ha, Jinse Park, Sung Eun Kim
Korean J Clin Neurophysiol. 2013;15(1):24-26. doi: 10.14253/kjcn.2013.15.1.24.
Reference
-
1. Onesti ST, Wisniewski T, Post KD. Pituitary hemorrhage into a Rathke's cleft cyst. Neurosurgery. 1990. 27:644–646.
Article2. Reid RL, Quigley ME, Yen SS. Pituitary apoplexy. A review. Arch Neurol. 1985. 42:712–719.3. Wakai S, Fukushima T, Teramoto A, Sano K. Pituitary apoplexy: its incidence and clinical significance. J Neurosurg. 1981. 55:187–193.
Article4. Mohr G, Hardy J. Hemorrhage, necrosis, and apoplexy in pituitary adenomas. Surg Neurol. 1982. 18:181–189.
Article5. Reutens DC, Edis RH. Pituitary apoplexy presenting as aseptic meningitis without visual loss or ophthalmoplegia. Aust N Z J Med. 1990. 20:590–591.
Article6. Valente M, Marroni M, Stagni G, Floridi P, Perriello G, Santeusanio F. Acute sterile meningitis as a primary manifestation of pituitary apoplexy. J Endocrinol Invest. 2003. 26:754–757.
Article7. Brouns R, Crols R, Engelborghs S, De Deyn PP. Pituitary apoplexy presenting as chemical meningitis. Lancet. 2004. 364:502.
Article8. Kim SY, Jung YS. Pituitary apoplexy presenting as meningitis. J Korean Soc Emerg Med. 2002. 13:94–96.9. Akutsu H, Noguchi S, Tsunoda T, Sasaki M, Matsumura A. Cerebral infarction following pituitary apoplexy--case report. Neurol Med Chir (Tokyo). 2004. 44:479–483.
Article10. Clark JD, Freer CE, Wheatley T. Pituitary apoplexy: an unusual cause of stroke. Clin Radiol. 1987. 38:75–77.11. Rosenbaum TJ, Houser OW, Laws ER. Pituitary apoplexy producing internal carotid artery occlusion. Case report. J Neurosurg. 1977. 47:599–604.12. Lath R, Rajshekhar V. Massive cerebral infarction as a feature of pituitary apoplexy. Neurol India. 2001. 49:191–193.13. Satyarthee GD, Mahapatra AK. Pituitary apoplexy in a child presenting with massive subarachnoid and intraventricular hemorrhage. J Clin Neurosci. 2005. 12:94–96.
Article14. Pozzati E, Frank G, Nasi MT, Giuliani G. Pituitary apoplexy, bilateral carotid vasospasm, and cerebral infarction in a 15-year-old boy. Neurosurgery. 1987. 20:56–59.
Article15. Semple PL, Webb MK, de Villiers JC, Laws ER Jr. Pituitary apoplexy. Neurosurgery. 2005. 56:65–72.
Article16. Dubuisson AS, Beckers A, Stevenaert A. Classical pituitary tumour apoplexy: Clinical features, management and outcomes in a series of 24 patients. Clin Neurol Neurosurg. 2007. 109:63–70.
Article17. Ebersold MJ, Laws ER Jr, Scheithauer BW, Randall RV. Pituitary apoplexy treated by transsphenoidal surgery. A clinicopathological and immunocytochemical study. J Neurosurg. 1983. 58:315–320.18. Nishioka H, Ito H, Haraoka J. Cerebral vasospasm following transsphenoidal removal of a pituitary adenoma. Br J Neurosurg. 2001. 15:44–47.19. Cardoso ER, Peterson EW. Pituitary apoplexy and vasospasm. Surg Neurol. 1983. 20:391–395.
Article20. Camp PE, Paxton HD, Buchan GC, Gahbauer H. Vasospasm after trans-sphenoidal hypophysectomy. Neurosurgery. 1980. 7:382–386.
Article21. Mukherjee S, Majumder A, Dattamunshi AK, Maji D. Ischaemic stroke leading to left hemiparesis and autohypophysectomy in a case of pituitary macroadenoma. J Assoc Physicians India. 1995. 43:801–802.22. Rovit RL, Fein JM. Pituitary apoplexy: a review and reappraisal. J Neurosurg. 1972. 37:280–288.
Article23. Mawk JR, Ausman JI, Erickson DL, Maxwell RE. Vasospasm following transcranial removal of large pituitary adenomas. Report of three cases. J Neurosurg. 1979. 50:229–232.24. Aoki N, Origitano TC, al-Mefty O. Vasospasm after resection of skull base tumors. Acta Neurochir (Wien). 1995. 132:53–58.
Article25. Wakai S, Fukushima T, Furihata T, Sano K. Association of cerebral aneurysm with pituitary adenoma. Surg Neurol. 1979. 12:503–507.26. Semple PL, De Villiers JC, Bowen RM, Lopes MB, Laws ER Jr. Pituitary apoplexy: do histological features influence the clinical presentation and outcome. J Neurosurg. 2006. 104:931–937.
Article
