Korean J Obstet Gynecol.
2012 Jun;55(6):403-407. 10.5468/KJOG.2012.55.6.403.
Conservative management of placenta increta treated with selective uterine artery embolization: Review of two cases
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Chonbuk National University Medical School, Jeonju, Korea. binnayokr@jbnu.ac.kr
- KMID: 1783933
- DOI: http://doi.org/10.5468/KJOG.2012.55.6.403
Abstract
- Placenta increta is a condition characterized by abnormal adherence of the placenta owing to entire or partial absence of the decidua basalis. It is generally recognized during difficult placental removal at the time of delivery. It is a life-threatening complication of pregnancy due to massive hemorrhage, uterine perforation, and infection and thus often a hysterectomy is required. We review two cases of placenta increta conservative managed successfully by selective uterine artery embolization.
MeSH Terms
Figure
-
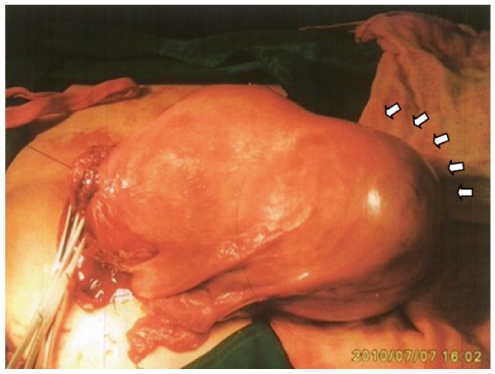
Fig. 1 Uterine abnormal bulging during Cesarean section (arrows).
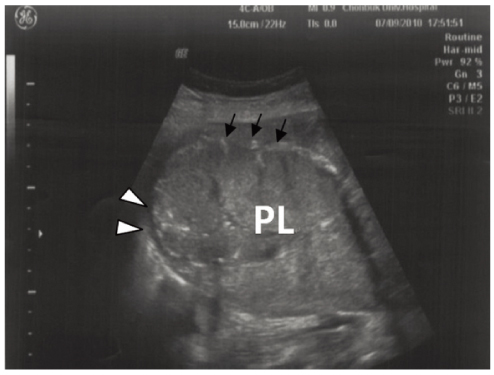
Fig. 2 Ultrasound examination obtained 2 days postoperation shows a thin uterine wall (arrowheads) at fundus of uterus and the loss of the echolucent space behind the placenta (PL) (arrows).

Fig. 3 View of uterus after baby out during Cesarean section: an enlarged uterus with extension out towards the left cornu (arrows).
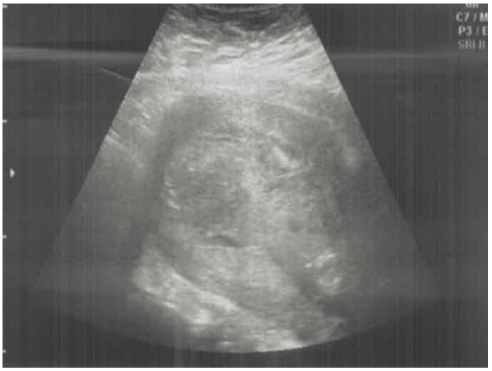
Fig. 4 Ultrasound examination showed the left uterine wall was deeply invaded by the placenta.
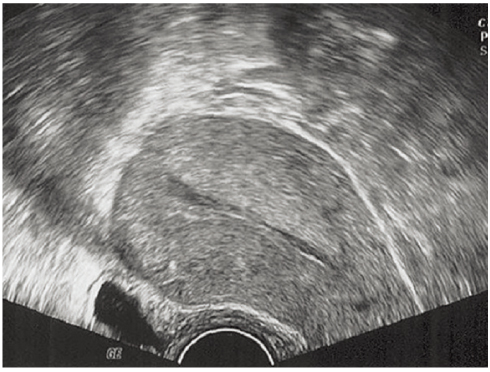
Fig. 5 Transvaginal sonogram 4 weeks after operation showed a thin linear endometrial cavity and no remnant placental tissue.
Reference
-
1. Berchuck A, Sokol RJ. Previous cesarean section, placenta increta, and uterine rupture in second-trimester abortion. Am J Obstet Gynecol. 1983. 145:766–767.2. Breen JL, Neubecker R, Gregori CA, Franklin JE Jr. Placenta accreta, increta, and percreta. A survey of 40 cases. Obstet Gynecol. 1977. 49:43–47.3. Committee on Obstetric Practice. ACOG committee opinion. Placenta accreta. Number 266, January 2002. American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet. 2002. 77:77–78.4. Miller DA, Chollet JA, Goodwin TM. Clinical risk factors for placenta previa-placenta accreta. Am J Obstet Gynecol. 1997. 177:210–214.5. Gielchinsky Y, Rojansky N, Fasouliotis SJ, Ezra Y. Placenta accreta: summary of 10 years: a survey of 310 cases. Placenta. 2002. 23:210–214.6. Suh YH, Song EH, Kim DH, Lee YH, Park HY, Koh KS, et al. A clinical study of placental adhesions: placenta accreta, placenta increta, and placenta percreta. Korean J Obstet Gynecol. 2003. 46:81–88.7. Levine D, Hulka CA, Ludmir J, Li W, Edelman RR. Placenta accreta: evaluation with color Doppler US, power Doppler US, and MR imaging. Radiology. 1997. 205:773–776.8. Legro RS, Price FV, Hill LM, Caritis SN. Nonsurgical management of placenta percreta: a case report. Obstet Gynecol. 1994. 83:847–849.9. Arulkumaran S, Ng CS, Ingemarsson I, Ratnam SS. Medical treatment of placenta accreta with methotrexate. Acta Obstet Gynecol Scand. 1986. 65:285–286.10. Henrich W, Fuchs I, Ehrenstein T, Kjos S, Schmider A, Dudenhausen JW. Antenatal diagnosis of placenta percreta with planned in situ retention and methotrexate therapy in a woman infected with HIV. Ultrasound Obstet Gynecol. 2002. 20:90–93.11. Mussalli GM, Shah J, Berck DJ, Elimian A, Tejani N, Manning FA. Placenta accreta and methotrexate therapy: three case reports. J Perinatol. 2000. 20:331–334.12. Brown BJ, Heaston DK, Poulson AM, Gabert HA, Mineau DE, Miller FJ Jr. Uncontrollable postpartum bleeding: a new approach to hemostasis through angiographic arterial embolization. Obstet Gynecol. 1979. 54:361–365.13. Descargues G, Douvrin F, Degré S, Lemoine JP, Marpeau L, Clavier E. Abnormal placentation and selective embolization of the uterine arteries. Eur J Obstet Gynecol Reprod Biol. 2001. 99:47–52.14. Timmermans S, van Hof AC, Duvekot JJ. Conservative management of abnormally invasive placentation. Obstet Gynecol Surv. 2007. 62:529–539.15. Kayem G, Davy C, Goffinet F, Thomas C, Clément D, Cabrol D. Conservative versus extirpative management in cases of placenta accreta. Obstet Gynecol. 2004. 104:531–536.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Placenta Increta in the Uterine Sacculation which was Treated with Conservative Methods
- One Case of Placenta Accreta Treated with Selective Uterine Artery Embolization Followed by Methotrexate
- Placenta Increta Presenting as Postabortal Uterine Mass in the First Trimester: A Case Report
- One case of placenta increta successfully treated with methotrexate
- A Case of Placenta Increta Successfully Treated with Methotrexate and Misoprostol
