Korean J Obstet Gynecol.
2012 Jun;55(6):371-377. 10.5468/KJOG.2012.55.6.371.
Quality of life according to add-back therapy during GnRH agonist treatment in endometriosis patients
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Pusan National University School of Medicine, Busan, Korea. ghkim@pusan.ac.kr
- KMID: 1783928
- DOI: http://doi.org/10.5468/KJOG.2012.55.6.371
Abstract
OBJECTIVE
This study was performed to investigate the effect of add-back therapy on quality of life during postoperative gonadotropin-releasing hormone (GnRH) agonist therapy for endometriosis.
METHODS
Fifty-one patients who were diagnosed as stage III/IV endometriosis after laparoscopic ovarian cystectomy from January 2009 to December 2010 were divided into GnRH agonist with add-back therapy group and GnRH agonist only group. Add-back therapy was started before third injection of GnRH agonist. Short form health survey (SF-36) instrument was checked preoperatively, at the time of 6th GnRH agonist therapy and 6 months after GnRH agonist therapy.
RESULTS
There were no differences between two groups on the mean age, body mass index and revised American Fertility Society score. In most cases, add-back therapy was added because of menopausal symptoms. Pelvic pain and dysmenorrhea showed no differences between two groups on each survey period. At the time of 6th GnRH agonist therapy, physical function in add-back therapy group was improved significantly compared with preoperative period (85.7+/-8.8 vs. 91.0+/-10.4, P=0.011). In GnRH only group, physical function at preoperative period was rather higher than at the time of 6th GnRH agonist therapy.
CONCLUSION
Add-back therapy during postoperative GnRH agonist therapy showed no negative effect on pelvic pain and dysmenorrhea. Physical function was improved in add back group. Add-back therapy might have an influence on quality of life in patients receiving postoperative GnRH agonist therapy for endometriosis.
Keyword
MeSH Terms
Figure
-
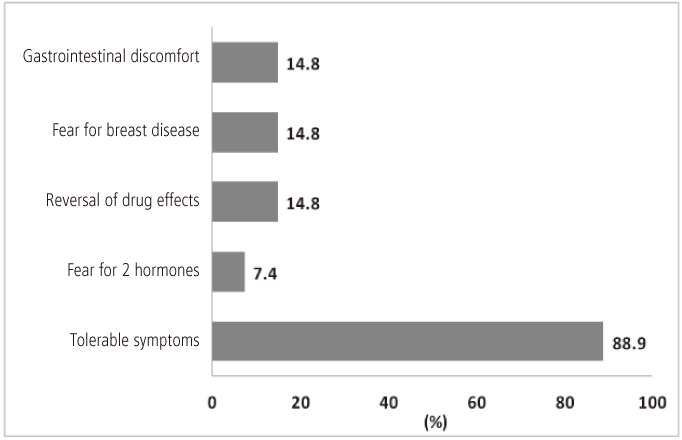
Fig. 1 Causes of no add-back therapya (n = 27). aMultiple causes included.
Reference
-
1. Olive DL, Schwartz LB. Endometriosis. N Engl J Med. 1993. 328:1759–1769.2. Park HM, Lee WS, Song MS, Hur M. The effect of progesterone add-back therapy on skeletal status during GnRH agonist therapy for endometriosis. Korean J Obstet Gynecol. 2003. 46:288–295.3. Batzer FR. GnRH analogs: options for endometriosis-associated pain treatment. J Minim Invasive Gynecol. 2006. 13:539–545.4. Olive DL. Gonadotropin-releasing hormone agonists for endometriosis. N Engl J Med. 2008. 359:1136–1142.5. Kiilholma P, Tuimala R, Kivinen S, Korhonen M, Hagman E. Comparison of the gonadotropin-releasing hormone agonist goserelin acetate alone versus goserelin combined with estrogen-progestogen add-back therapy in the treatment of endometriosis. Fertil Steril. 1995. 64:903–908.6. Fernandez H, Lucas C, Hédon B, Meyer JL, Mayenga JM, Roux C. One year comparison between two add-back therapies in patients treated with a GnRH agonist for symptomatic endometriosis: a randomized double-blind trial. Hum Reprod. 2004. 19:1465–1471.7. Friedman AJ, Hornstein MD. Gonadotropin-releasing hormone agonist plus estrogen-progestin "add-back" therapy for endometriosis-related pelvic pain. Fertil Steril. 1993. 60:236–241.8. McHorney CA, Ware JE Jr, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care. 1993. 31:247–263.9. Jenkinson C, Coulter A, Wright L. Short form 36 (SF36) health survey questionnaire: normative data for adults of working age. BMJ. 1993. 306:1437–1440.10. Valle RF, Sciarra JJ. Endometriosis: treatment strategies. Ann N Y Acad Sci. 2003. 997:229–239.11. Jee BC, Lee JY, Suh CS, Kim SH, Choi YM, Moon SY. Impact of GnRH agonist treatment on recurrence of ovarian endometriomas after conservative laparoscopic surgery. Fertil Steril. 2009. 91:40–45.12. Barbieri RL. Hormone treatment of endometriosis: the estrogen threshold hypothesis. Am J Obstet Gynecol. 1992. 166:740–745.13. Fuldeore MJ, Marx SE, Chwalisz K, Smeeding JE, Brook RA. Add-back therapy use and its impact on LA persistence in patients with endometriosis. Curr Med Res Opin. 2010. 26:729–736.14. Olive DL. The role of add-back therapy in the United States. Drugs Today (Barc). 2005. 41:Suppl A. 23–26.15. Zupi E, Marconi D, Sbracia M, Zullo F, De Vivo B, Exacustos C, et al. Add-back therapy in the treatment of endometriosis-associated pain. Fertil Steril. 2004. 82:1303–1308.16. Surrey ES. Add-Back Consensus Working Group. Add-back therapy and gonadotropin-releasing hormone agonists in the treatment of patients with endometriosis: can a consensus be reached? Fertil Steril. 1999. 71:420–424.17. Kim NY, Ryoo U, Lee DY, Kim MJ, Yoon BK, Choi D. The efficacy and tolerability of short-term low-dose estrogen-only add-back therapy during post-operative GnRH agonist treatment for endometriosis. Eur J Obstet Gynecol Reprod Biol. 2011. 154:85–89.18. Morris EP, Rymer J, Robinson J, Fogelman I. Efficacy of tibolone as "add-back therapy" in conjunction with a gonadotropin-releasing hormone analogue in the treatment of uterine fibroids. Fertil Steril. 2008. 89:421–428.19. Surrey ES. Gonadotropin-releasing hormone agonist and add-back therapy: what do the data show? Curr Opin Obstet Gynecol. 2010. 22:283–288.20. Al-Azemi M, Jones G, Sirkeci F, Walters S, Houdmont M, Ledger W. Immediate and delayed add-back hormonal replacement therapy during ultra long GnRH agonist treatment of chronic cyclical pelvic pain. BJOG. 2009. 116:1646–1656.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effects of different add-back regimens on hypoestrogenic problems by postoperative gonadotropin-releasing hormone agonist treatment in endometriosis
- The Effect of Progestogen Add-back Therapy on Skeletal Status During GnRH Agonist Therapy for Endometriosis
- The usefulness of combined treatment of GnRH agonist and levonorgestrel-releasing intrauterine system (Mirena(R)) for chronic pelvic pain of endometriosis
- A case of pulmonary endometriosis presenting with catamenial pneumothorax
- The role of gonadotrophin releasing hormone agonist for the treatment of scar endometriosis
