Yonsei Med J.
2014 Jan;55(1):157-161. 10.3349/ymj.2014.55.1.157.
Clinical Characteristics and Management of Benign Transient Non-Organic Ileus of Neonates: A Single-Center Experience
- Affiliations
-
- 1Department of Surgery, Seoul St. Mary's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea.
- 2Department of Pediatrics, Severance Children's Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Pediatric Surgery, Severance Children's Hospital, Yonsei University College of Medicine, Seoul, Korea. jtoh@yuhs.ac
- KMID: 1779900
- DOI: http://doi.org/10.3349/ymj.2014.55.1.157
Abstract
- PURPOSE
The term benign transient non-organic ileus of neonates (BTNIN) is applied to neonates who present symptoms and plain radiographic findings of Hirschsprung's disease, but do not have aganglionic bowel and are managed well by conservative treatment. It can often be difficult to diagnose BTNIN because its initial symptoms are similar to those of Hirschsprung's disease. The aim of this study is to evaluate the clinical characteristics and proper treatment of BTNIN.
MATERIALS AND METHODS
A retrospective review was made on the clinical data of 19 neonates who were treated for BTNIN between January 2008 and December 2011 at a single facility.
RESULTS
Abdominal distension occurred in every patient (19/19). Other common symptoms included emesis (5/19), explosive defecation (5/19), and constipation (4/19). The vast majority of patients (15/19) experienced the onset of symptoms between 2 and 4 weeks of age. Radiograph findings from all of the patients were similar to Hirschsprung's disease. A barium study showed a transition zone in 33.4% (6/18) of the patients. However, rectal biopsy revealed ganglion cells in the distal rectum in 88.2% (15/17) of the patients, and anorectal manometry showed a normal rectoanal inhibitory reflex in 90% (9/10). All patients responded well to conservative treatment. Symptoms disappeared at the mean age of 4.9+/-1.0 months, and the abdominal radiographs normalized.
CONCLUSION
BTNIN had an excellent outcome with conservative treatment, and must be differentiated from Hirschsprung's disease. A rectal biopsy and anorectal manometry were useful diagnostic tools in the differential diagnosis.
Keyword
MeSH Terms
Figure
-
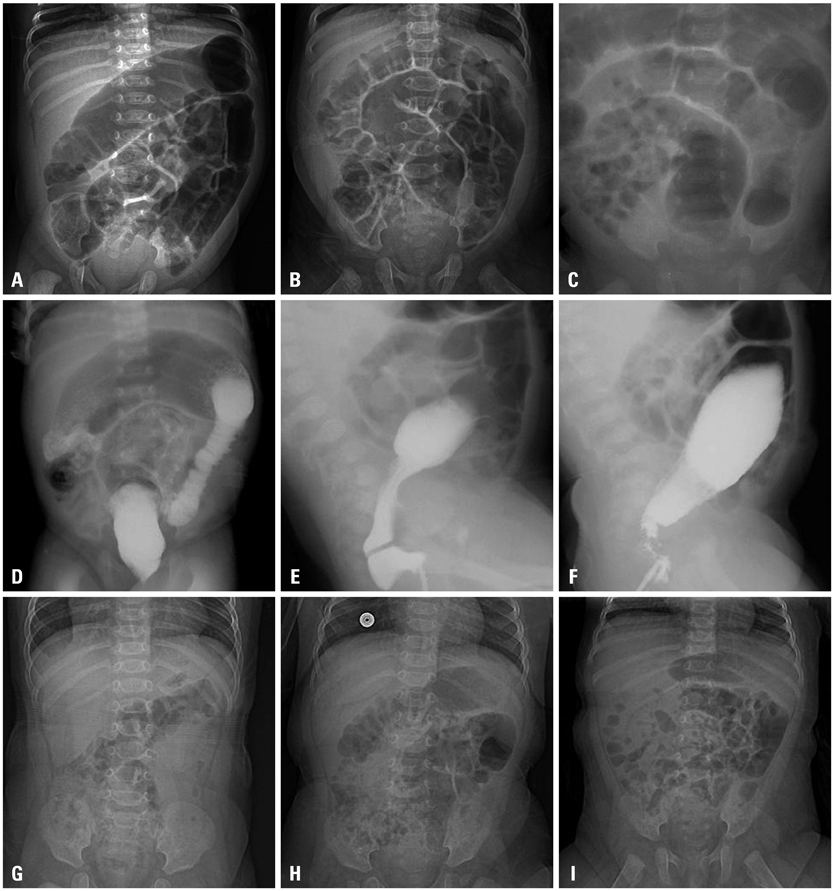
Fig. 1 Plain radiograph findings similar to Hirschsprung's disease appeared (A, B and C). Barium studies (D, E and F) showed transition zones. After conservative treatment, symptoms disappeared, and the radiographs normalized (G, H and I). Figures (A, D, F), (B, E, H) and (C, F, I) are taken from the same patients, respectively.
Reference
-
1. Haricharan RN, Georgeson KE. Hirschsprung disease. Semin Pediatr Surg. 2008; 17:266–275.
Article2. Puri P, Gosemann JH. Variants of Hirschsprung disease. Semin Pediatr Surg. 2012; 21:310–318.
Article3. Yamauchi K, Kubota A, Usui N, Yonekura T, Kosumi T, Nogami T, et al. Benign transient non-organic ileus of neonates. Eur J Pediatr Surg. 2002; 12:168–174.
Article4. Kubota A, Kawahara H, Okuyama H, Shimizu Y, Nakacho M, Ida S, et al. Cow's milk protein allergy presenting with Hirschsprung's disease-mimicking symptoms. J Pediatr Surg. 2006; 41:2056–2058.
Article5. Lee JH, Choe YH, Lee SK, Seo JM, Kim JH, Suh YL. Allergic proctitis and abdominal distention mimicking Hirschsprung's disease in infants. Acta Paediatr. 2007; 96:1784–1789.
Article6. Dasgupta R, Langer JC. Transanal pull-through for Hirschsprung disease. Semin Pediatr Surg. 2005; 14:64–71.
Article7. Kim HY, Oh JT. Stabilization period after 1-stage transanal endorectal pull-through operation for Hirschsprung disease. J Pediatr Surg. 2009; 44:1799–1804.
Article8. Langer JC, Durrant AC, de la Torre L, Teitelbaum DH, Minkes RK, Caty MG, et al. One-stage transanal Soave pullthrough for Hirschsprung disease: a multicenter experience with 141 children. Ann Surg. 2003; 238:569–583.9. de Lorijn F, Kremer LC, Reitsma JB, Benninga MA. Diagnostic tests in Hirschsprung disease: a systematic review. J Pediatr Gastroenterol Nutr. 2006; 42:496–505.10. Jamieson DH, Dundas SE, Belushi SA, Cooper M, Blair GK. Does the transition zone reliably delineate aganglionic bowel in Hirschsprung's disease? Pediatr Radiol. 2004; 34:811–815.
Article11. Lewis NA, Levitt MA, Zallen GS, Zafar MS, Iacono KL, Rossman JE, et al. Diagnosing Hirschsprung's disease: increasing the odds of a positive rectal biopsy result. J Pediatr Surg. 2003; 38:412–416.
Article12. Järvinen KM, Suomalainen H. Development of cow's milk allergy in breast-fed infants. Clin Exp Allergy. 2001; 31:978–987.
Article13. Burki T, Kiho L, Scheimberg I, Phelps S, Misra D, Ward H, et al. Neonatal functional intestinal obstruction and the presence of severely immature ganglion cells on rectal biopsy: 6 year experience. Pediatr Surg Int. 2011; 27:487–490.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Probability of Food Allergy in Case of Benign Transient Non-Organic Ileus of Neonate
- Transient Intestinal Ileus in Neonate: A Study of Comparison with Hirschsprung's Disease
- Comparison of Acute Abdominal Surgical Outcomes of Extremely-Low-Birth-Weight Neonates according to Differential Diagnosis
- Comparative Study on the Clinical Characteristics of Transient Tachypnea of Newborns according to the Need for Invasive Mechanical Ventilation
- Applying the Bacterial Meningitis Score in Neonates Diagnosed Meningitis: A Single Center Experience
