Risk Factors for Postoperative Complications after Open Infrarenal Abdominal Aortic Aneurysm Repair in Koreans
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hyunjooahn@skku.edu
- 2Department of Anesthesiology and Pain Medicine, Seoul Medical Center, Seoul, Korea.
- 3Biostatistics Unit, Samsung Biomedical Research Institute, Seoul, Korea.
- KMID: 1779673
- DOI: http://doi.org/10.3349/ymj.2011.52.2.339
Abstract
- PURPOSE
Open infrarenal abdominal aortic aneurysm (AAA) repair is performed without event in most cases. However, some patients suffer major morbidities such as renal failure, myocardial infarction, paraplegia, acute respiratory distress syndrome, or hepatic dysfunction. Predicting what kinds of patient populations are more prone to develop such complications may keep the clinicians more attentive to the patients, possibly leading to better prognoses. In this retrospective study, we searched the incidence of and risk factors for postoperative complications and their predictive equations in 162 patients who underwent open infrarenal AAA repair.
MATERIALS AND METHODS
Postoperative complications were observed within 30 days. Patient characteristics, types of aneurysm and surgery, and hemodynamic and metabolic variables during the periclamp period were analyzed in relation to postoperative complications using multiple logistic regression analysis.
RESULTS
Postoperative complications involved the cardiac (20%), pulmonary (14%), renal (13%), gastrointestinal (6%), hepatic (3.1%), and neurologic (2.5%) systems, and bleeding occurred in 1.2% of cases. The mortality rate was 5.6%. The risk factors were age [> 67 yrs, odds ratio (OR) 2.6], clamp duration (> 110 min, OR 4.7), volume of blood transfusion (> 1,280 mL, OR 4.4), emergency operation (OR 1.4), and vasopressor infusion during clamp (OR 1.4). The prediction model was: P(x) = exp(alpha)/[1 + exp(alpha)] alpha;-2.2 + 0.9 x age + 1.5 x clamp duration + 1.5 x transfusion + 0.3 x emergency + 0.4 x vasopressor infusion [insert 1 if risk factors exist, otherwise, insert 0 to each variable].
CONCLUSION
A significant number of complications occurred after infrarenal AAA repair. Therefore, creating a protocol to identify and monitor high risk patients would improve postoperative care.
MeSH Terms
Figure
-
Fig. 1 Flow diagram of patient inclusion.
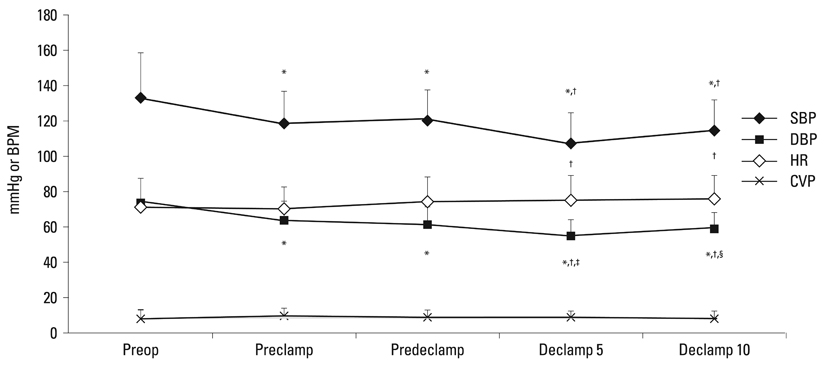
Fig. 2 Hemodynamic changes during the operation. SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; CVP, central venous pressure; Declamp 5, 5 min after declamp; Declamp 10, 10 min after declamp; BPM, beat per minute. *p < 0.05 compared to Preop. †p < 0.05 compared to Preclamp. ‡p < 0.05 compared to Predeclamp. §p < 0.05 campared to Declamp 5.
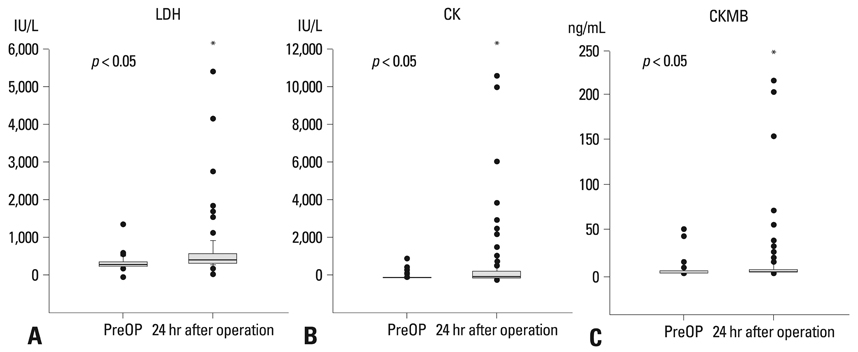
Fig. 3 Box plot of LDH, CK, and CKMB. *p < 0.05 compard to PreOP. LDH, lactate dehydorgenase; CK, creatine kinase; CKMB, creatine kinase isoenzyme.
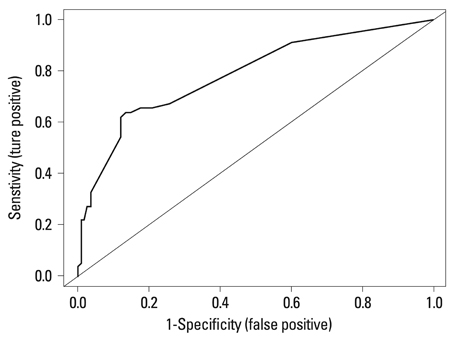
Fig. 4 The area under the receiver operating characteristic (ROC) curve. The AUC value was 0.78 (95% CI 0.71-0.85) for this model. AUC, area under the curve; CI, confidence interval.
Reference
-
1. Scott RA, Vardulaki KA, Walker NM, Day NE, Duffy SW, Ashton HA. The long-term benefits of a single scan for abdominal aortic aneurysm (AAA) at age 65. Eur J Vasc Endovasc Surg. 2001. 21:535–540.
Article2. Lawrence PF, Gazak C, Bhirangi L, Jones B, Bhirangi K, Oderich G, et al. The epidemiology of surgically repaired aneurysms in the United States. J Vasc Surg. 1999. 30:632–640.
Article3. Bayly PJ, Matthews JN, Dobson PM, Price ML, Thomas DG. In-hospital mortality from abdominal aortic surgery in Great Britain and Ireland: Vascular Anaesthesia Society audit. Br J Surg. 2001. 88:687–692.
Article4. Back MR, Bandyk M, Bradner M, Cuthbertson D, Johnson BL, Shames ML, et al. Critical analysis of outcome determinants affecting repair of intact aneurysms involving the visceral aorta. Ann Vasc Surg. 2005. 19:648–656.
Article5. McArdle GT, Price G, Lewis A, Hood JM, McKinley A, Blair PH, et al. Positive fluid balance is associated with complications after elective open infrarenal abdominal aortic aneurysm repair. Eur J Vasc Endovasc Surg. 2007. 34:522–527.
Article6. Hertzer NR, Mascha EJ. A personal experience with factors influencing survival after elective open repair of infrarenal aortic aneurysms. J Vasc Surg. 2005. 42:898–905.
Article7. Carvalho FC, Brito VP, Tribulatto EC, van Bellen B. [Prospective study of early and late morbidity and mortality in the abdominal aortic aneurysm surgical repair]. Arq Bras Cardiol. 2005. 84:292–296.8. Adembri C, Kastamoniti E, Bertolozzi I, Vanni S, Dorigo W, Coppo M, et al. Pulmonary injury follows systemic inflammatory reaction in infrarenal aortic surgery. Crit Care Med. 2004. 32:1170–1177.
Article9. Fantini GA, Conte MS. Pulmonary failure following lower torso ischemia: clinical evidence for a remote effect of reperfusion injury. Am Surg. 1995. 61:316–319.10. Huber TS, Harward TR, Flynn TC, Albright JL, Seeger JM. Operative mortality rates after elective infrarenal aortic reconstructions. J Vasc Surg. 1995. 22:287–293.
Article11. Yassin MM, Barros D'Sa AA, Parks TG, McCaigue MD, Leggett P, Halliday MI, et al. Lower limb ischaemia-reperfusion injury alters gastrointestinal structure and function. Br J Surg. 1997. 84:1425–1429.
Article12. Neary P, Hurson C, Briain DO, Brabazon A, Mehigan D, Keaveny TV, et al. Abdominal aortic aneurysm repair and colonic infarction: a risk factor appraisal. Colorectal Dis. 2007. 9:166–172.
Article13. Malinzak LE, Long GW, Bove PG, Brown OW, Romano W, Shanley CJ, et al. Gastrointestinal complications following infrarenal endovascular aneurysm repair. Vasc Endovascular Surg. 2004. 38:137–142.
Article14. Colson P, Ribstein J, Séguin JR, Marty-Ane C, Roquefeuil B. Mechanisms of renal hemodynamic impairment during infrarenal aortic cross-clamping. Anesth Analg. 1992. 75:18–23.
Article15. Gamulin Z, Forster A, Morel D, Simonet F, Aymon E, Favre H. Effects of infrarenal aortic cross-clamping on renal hemodynamics in humans. Anesthesiology. 1984. 61:394–399.
Article16. Alpagut U, Dayioglu E. Anterior spinal artery syndrome after infrarenal abdominal aortic surgery. J Cardiovasc Surg (Torino). 2002. 43:865–868.17. Dougherty MJ, Calligaro KD. How to avoid and manage nerve injuries associated with aortic surgery: ischemic neuropathy, traction injuries, and sexual derangements. Semin Vasc Surg. 2001. 14:275–281.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Novel Technique to Rescue a Folded Aortic Endograft during Endovascular Aneurysm Repair
- Ruptured Abdominal Aortic Aneurysm with Antecedent Endovascular Repair of Abdominal Aortic Aneurysm
- The Complications and Their Management after Endovascular Aneurysm Repair for the Treatment of Abdominal Aortic Aneurysms
- Endovascular Stent-Graft Placement and Secondary Intervention for Abdominal Aortic Aneurysm in a Patient who had a Previously Inserted Iliac Stent
- Open Repair of Ruptured Huge Aorto-Iliac Aneurysm: Warning of Colon Ischemia
