Balloon Valvuloplasty for Neonatal Critical Pulmonary Valvar Stenosis with IVC Interruption: Pitfalls of the Transumbilical Approach
- Affiliations
-
- 1Department of Pediatrics, Seoul National University Children's Hospital, Seoul, Korea. eunjbaek@snu.ac.kr
- KMID: 1778049
- DOI: http://doi.org/10.3346/jkms.2010.25.3.485
Abstract
- Transcatheter balloon pulmonary valvuloplasty (BPV) is considered to be the treatment of choice for neonates with critical pulmonary valvar stenosis (PVS) or pulmonary valvar atresia with intact ventricular septum accompanied by reasonable right ventricular volume. The percutaneous femoral venous access is the most preferred route for BPV in most cardiac centers. We report herein the case of a newborn baby with critical PVS with inferior vena cava interruption, severe tricuspid regurgitation and a severely enlarged right atrium. We tried BPV through the transumbilical approach with difficulty, but he was successfully treated with the assistance of a coronary artery guiding catheter.
MeSH Terms
Figure
-
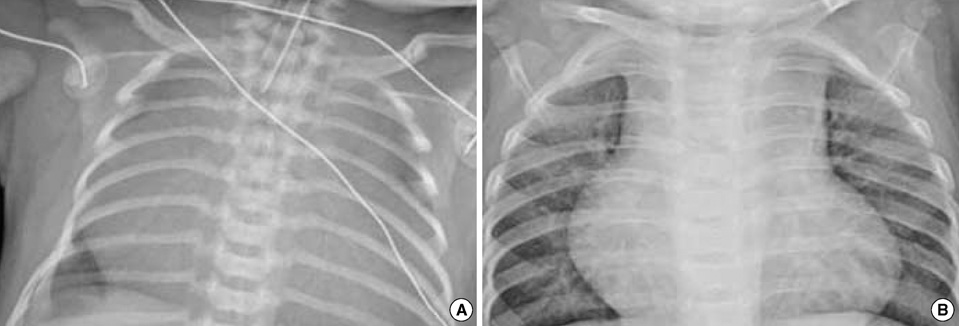
Fig. 1 Changes in heart size before (A) and after (B) balloon pulmonary valvuloplasty. Marked cardiomegaly regressed nine months after successful valvuloplasty on chest radiography.
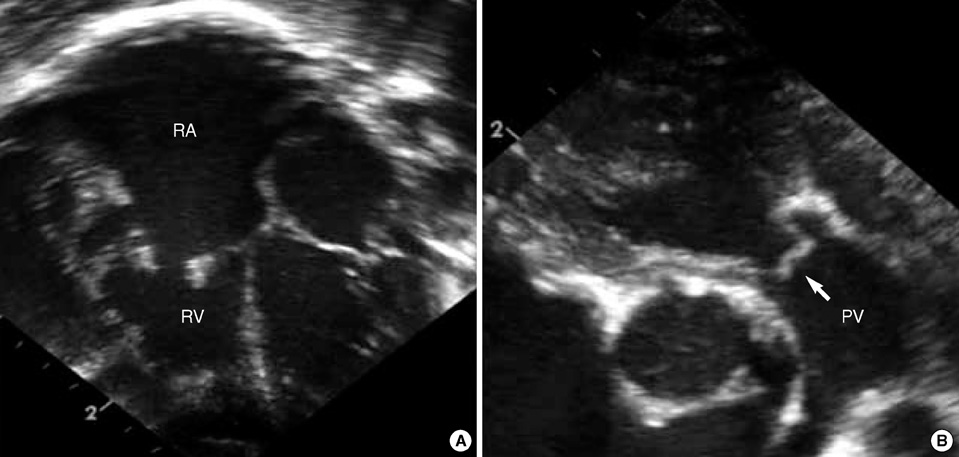
Fig. 2 Echocardiographic findings before balloon pulmonary valvuloplasty. Trans-thoracic echocardiograms showed a severely enlarged right atrium (RA), a relatively small right ventricle (RV) (A), a thickened tricuspid valve and a pinhole pulmonary valvar orifice with doming of leaflets (B). PV, pulmonary valve.
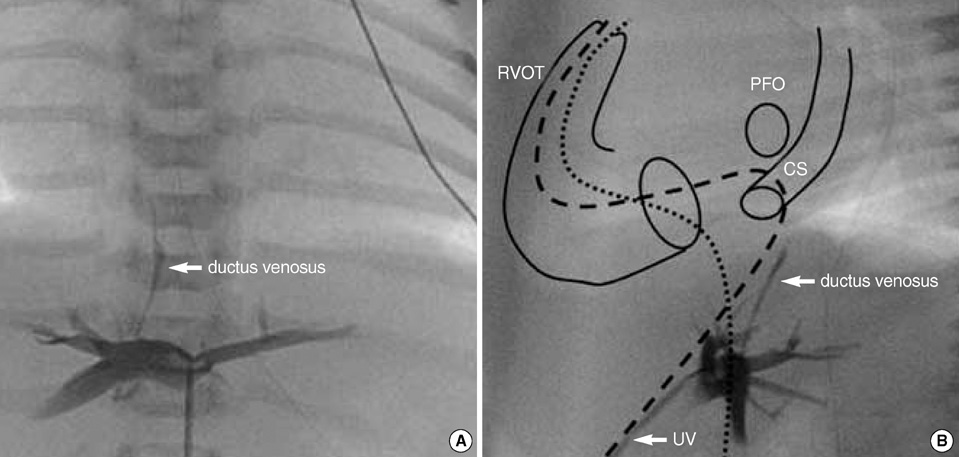
Fig. 3 Anteroposterior (A) and lateral (B) view of umbilical venous angiography. (A) Angiography of the umbilical vein (UV) showed a stenotic or nearly closing ductus venosus. (B) Catheter introduction to the right ventricular and right ventricular outlet tracts (RVOTs) was extremely difficult and very different from the transfemoral approach (thin dotted line) because posteriorly deviated sheath (thick dotted line) made the catheter easily go into patent foramen ovale (PFO) or coronary sinus (CS).
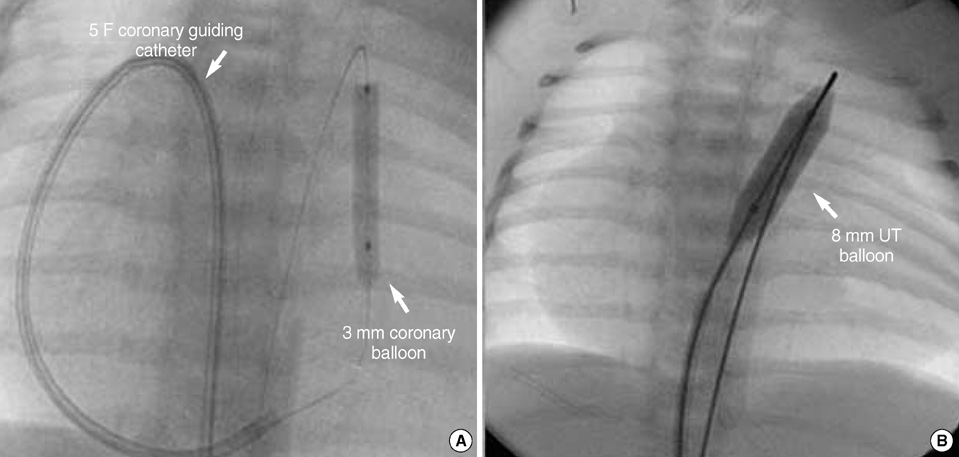
Fig. 4 Successful balloon valvuloplasty for pulmonary valvar stenosis. (A) Successful ballooning of a 3-mm diameter coronary balloon catheter with the assistance of a 5F right coronary artery guiding catheter formed a loop within the right atrium. (B) Sequential dilatation of pulmonary valve with an 8-mm diameter Ultra-thin (UT) balloon catheter.
Reference
-
1. Kan JS, White RI Jr, Mitchell SE, Gardner TJ. Percutaneous balloon valvuloplasty: a new method for treating congenital pulmonary-valve stenosis. N Engl J Med. 1982. 30:540–542.
Article2. Weber HS. Initial and late results after catheter intervention for neonatal critical pulmonary valve stenosis and atresia with intact ventricular septum: a technique in continual evolution. Catheter Cardiovasc Interv. 2002. 56:394–399.
Article3. Shim D, Lloyd TR, Cho KJ, Moorehead CP, Beekman RH 3rd. Transhepatic cardiac catheterization in children. Evaluation of efficacy and safety. Circulation. 1995. 9:1526–1530.4. Chaara A, Zniber L, el Haitem N, Benomar M. Percutaneous balloon valvuloplasty via the right internal jugular vein for valvular pulmonic stenosis with severe right ventricular failure. Am Heart J. 1989. 117:684–685.
Article5. Meyer WW, Lind J. The ductus venosus and the mechanism of its closure. Arch Dis Child. 1966. 41:597–605.
Article6. Linde LM, Higashino SM, Berman G, Sapin SO, Emmanouilides GC. Umbilical vessel cardiac catheterization and angiocardiography. Circulation. 1966. 34:984–988.
Article7. Abinader E, Zeltzer M, Riss E. Transumbilical atrial septostomy in the newborn. Am J Dis Child. 1970. 119:354–355.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous transluminal balloon valvuloplasty for congenital pulmonary valvular stenosis
- Percutaneous transluminal balloon valvuloplasty for congenital pulmonary valve stenosis and aortic valve stenosis
- Percutaneous Transluminal Balloon Valvuloplasty for Congenital Pulmonary Valve Stenosis
- Percutaneous Balloon Valvuloplasty with Trefoil Balloon Catheter for the Treatment of Congenital Pulmonary Stenosis in Children
- A Case of Balloon Valvuloplasty using Three Balloon Catheters in a Child with Pulmonic Stenosis
