Usefulness of MR Imaging for Diseases of the Small Intestine: Comparison with CT
- Affiliations
-
- 1Department of Diagnostic Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 1777295
- DOI: http://doi.org/10.3348/kjr.2000.1.1.43
Abstract
OBJECTIVE
To evaluate the usefulness of MR imaging for diseases of the small intestine, emphasizing a comparison with CT. MATERIALS AND METHODS: Thirty-four patients who underwent both CT and MR imaging using FLASH 2D and HASTE sequences were analyzed. All patients had various small bowel diseases with variable association of peritoneal lesions. We compared the detectabilities of CT and MR imaging using different MR pulse sequences. The capability for analyzing the characteristics of small intestinal disease was also compared. RESULTS: MR imaging was nearly equal to CT for detecting intraluminal or peritoneal masses, lesions in the bowel and mesentery, and small bowel obstruction, but was definitely inferior for detecting omental lesions. The most successful MR imaging sequence was HASTE for demonstrating bowel wall thickening, coronal FLASH 2D for mesenteric lesions, and axial FLASH 2D for omental lesions. MR imaging yielded greater information than CT in six of 12 inflammatory bowel diseases, while it was equal to CT in six of seven neoplasms and inferior in five of seven mesenteric ischemia. In determining the primary causes of 15 intestinal obstructions, MR imaging was correct in 11 (73%) and CT in nine (60%) patients. CONCLUSION: MR imaging can serve as an alternative diagnostic tool for patients with suspected inflammatory bowel disease, small intestinal neoplasm or obstruction. is a high-speed, heavily T2-weighted sequence with a great sensitivity for fluid (11). This advance may make it possible to use breath-hold turbo spin-echo MR.
Keyword
MeSH Terms
Figure
-

Fig. 1 Intestinal ischemia in a 74-year-old man. A. Contrast-enhanced CT scan shows bowel wall thickening with a target sign (arrows). Note regional mesenteric haziness and vascular engorgement (arrowheads). B. Coronal HASTE MR image shows target sign in thickened bowel wall (arrows).
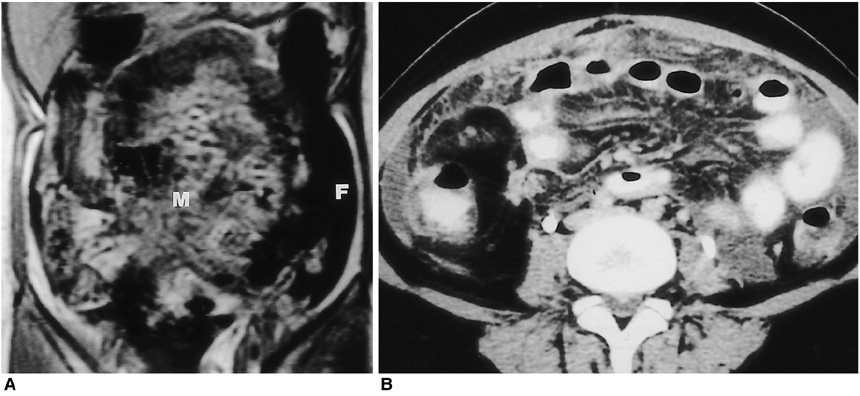
Fig. 2 Tuberculous peritonitis in a 24-year-old woman. A. Coronal FLASH 2D MR image shows miliary implants scattered in the mesentery (M). A loculated intraperitoneal fluid collection (F) is also noted. B. Contrast-enhanced CT scan shows better visualization of miliary lesions in the greater omentum and mesentery as well as ascites.

Fig. 3 A 35-year-old man with Crohn s disease. A. Coronal HASTE MR image demonstrates eccentric bowel wall thickening along mesenteric borders (arrows) of the bowel loops. Note bowel separation due to fibrofatty proliferation (arrowheads). B. Small bowel follow through shows marginal ulcer (arrowheads) along the mesenteric border of the small intestine. Note inflammatory stricture (arrows) of pelvic bowel loop along with regional bowel separation due to inflammatory infiltrates and fibrofatty proliferation.

Fig. 4 Leiomyosarcoma of the jejunum in a 71-year-old man. A. Contrast-enhanced CT scan shows a poorly enhanced soft tissue mass (*) in the pelvis, partially attaching to the adjacent bowel. B. Coronal HASTE MR image shows a hyperintense soft tissue mass (straight arrows). In contrast to CT image (A), lobulated configuration is well demonstrated on this image. Intestinal loop (curved arrow) is entrapped within the mass lesion.

Fig. 5 Intestinal lymphoma developing intussusception in a 30-year-old woman. A. Contrast-enhanced CT scan shows minimal bowel wall thickening (arrows) in the contrast-filled small intestinal loops as well as evidence of intussusception (*). At surgery, intussusception developed secondary to a polypoid intraluminal mass in the ileum. B. Coronal HASTE MR image also shows intussusception (arrows) and minimal bowel wall thickening (arrowheads).
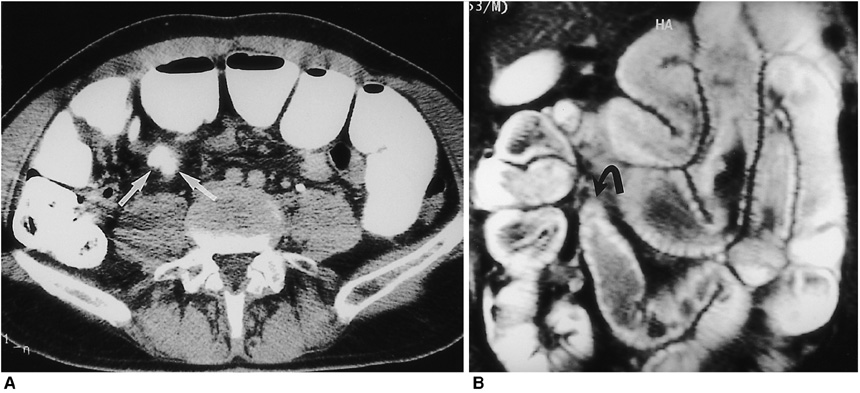
Fig. 6 Simple intestinal obstruction due to bowel adhesions in a 55-year-old man. A. Contrast-enhanced CT scan shows end-on view of narrowed intestinal segment (arrows) just proximal to the obstructed site. B. Coronal HASTE MR image shows diffuse dilatation of small intestinal loop with tapered narrowing at the obstructed site (curved arrow).
Reference
-
1. Chou CK, Chen LT, Sheu RS, Wang ML, Jaw TS, Liu GC. MRI manifestations of gastrointestinal wall thickening. Abdom Imaging. 1994. 19:389–394.2. Chou CK, Chen LT, Sheu RS, et al. MRI manifestations of gastrointestinal lymphoma. Abdom Imaging. 1994. 19:495–500.3. Ha HK, Lee EH, Lim CH, et al. Application of MRI for small intestinal diseases. J Magn Reson Imaging. 1998. 8:375–383.4. Madsen SM, Thomsen HS, Munkholm P, Schlichting P, Davidsen B. Magnetic resonance imaging of Crohn disease: early recognition of treatment response and relapse. Abdom Imaging. 1997. 22:164–166.5. Beers BV, Grandin C, Kartheuser A, et al. MRI of complicated anal fistulae: comparison with digital examination. J Comput Assist Tomogr. 1994. 18:87–90.6. Regan F, Bohlman ME, Khazan R, Rodriguez R, Schultze-Haaakh H. MR urography using HASTE imaging in the assessment of ureteric obstruction. AJR. 1996. 167:1115–1120.7. Aerts P, Hoe LV, Bosmans H, Oyen R, Marchal G, Baert AL. Breath-hold MR urography using the HASTE technique. AJR. 1996. 166:543–545.8. Miyazaki T, Yamashita Y, Tsuchigame T, Yamamoto H, Urata J, Takahashi M. MR cholangiopancreatography using HASTE (half-Fourier acquisition single-shot turbo spin-echo) sequences. AJR. 1996. 166:1297–1303.9. Tang Y, Yamashita Y, Namimoto T, et al. The value of MR urography that uses HASTE sequences to reveal urinary tract disorders. AJR. 1996. 167:1497–1502.10. Yamashita Y, Namimoto T, Abe Y, et al. MR imaging of the fetus by a HASTE sequence. AJR. 1997. 168:513–519.11. Regan F, Beall DP, Bohlman ME, et al. Fast MR imaging and the detection of small-bowel obstruction. AJR. 1998. 170:1465–1469.12. Fukuya T, Hawes DR, Lu CC, Chang PJ, Barloon TJ. CT diagnosis of small-bowel obstruction: efficacy in 60 patients. AJR. 1992. 158:765–769.13. Gazelle GS, Goldberg MA, Wittenberg J, Halpern EF, Pinkney L, Mueller PR. Efficacy of CT in distinguishing small-bowel obstruction from other causes of small-bowel dilatation. AJR. 1994. 162:43–47.14. Giovagnoni A, Misericordia M, Terilli F, Brunelli E, Contucci S, Bearzi I. MR imaging of ulcerative colitis. Abdom Imaging. 1993. 18:371–375.15. Auh YH, Lim T-H, Lee DH, et al. In Vitro MR imaging of the resected stomach with a 4.7-T superconducting magnet. Radiology. 1994. 191:129–134.16. Pattern RM, Moss AA, Fenton TA, Elliot S. OMR, A positive bowel contrast agent for abdominal and pelvic MR imaging: safety and imaging characteristics. J Magn Reson Imaging. 1992. 2:25–34.17. Patten RM, Lo SK, Philips JJ, et al. Positive bowel contrast agent for MR imaging of the abdomen: phase II and III clinical trials. Radiology. 1993. 189:277–283.18. Ros PR, Steinman RM, Torres GM, et al. The value of barium as a gastrointestinal contrast agent in MR imaging: a comparison study in normal volunteers. AJR. 1991. 157:761–767.19. Anderson CM, Brown JJ, Balfe DM, et al. MR imaging of Crohn disease: use of perflubron as a gastrointestinal contrast agent. J Magn Reson Imaging. 1994. 4:491–496.20. Hiraishi K, Narabayashi IN, Fujita O, et al. Blueberry juice: preliminary evaluation as an oral contrast agent in gastrointestinal MR imaging. Radiology. 1995. 194:119–123.21. Low RN, Sigeti JS. MR imaging of peritoneal disease: comparison of contrast-enhanced fast multiplanar spoiled gradient-recalled and spin-echo imaging. AJR. 1994. 163:1131–1140.22. Ha HK, Kim JS, Lee MS, et al. Differentiation of simple and strangulated small-bowel obstructions: usefulness of known CT criteria. Radiology. 1997. 204:507–512.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Preparation, Technique, and Imaging of Computed Tomography/Magnetic Resonance Enterography
- Detection of Acute Intraventricular Hemorrhage: Comparison of FLAIR MR Imaging with Unenhanced CT
- Incidentally Detected Small Intestine Intussusception Caused by Primary Small Intestine Carcinoma on ¹â¸F-FDG PET/CT
- Staging of uterine cervical carcinoma: comparison of CT and MR imaging
- Comparison of Fluid-Attenuated Inversion-Recovery Magnetic Resonance Imaging with Computed Tomography in Acute Intraventricular Hemorrhage
