Yonsei Med J.
2006 Dec;47(6):805-810. 10.3349/ymj.2006.47.6.805.
Endoscopic Papillary Balloon Dilation with Large Balloon after Limited Sphincterotomy for Retrieval of Choledocholithiasis
- Affiliations
-
- 1Division of Gastroenterology, Institute of Gastroenterology, Departments of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. jbchung@yumc.yonsei. ac.kr
- KMID: 1777169
- DOI: http://doi.org/10.3349/ymj.2006.47.6.805
Abstract
- Endoscopic papillary balloon dilation (EBD) for choledocholithiasis is known to be comparable to endoscopic sphincterotomy (EST) especially in cases of small stones. With larger stones, EBD with conventional balloon, which have a diameter of 6-8 mm, was reported as less effective for extraction of stones. We evaluated the efficacy and complications of EBD with large balloons (10-15 mm) after limited EST for retrieval of choledocholithiasis. From February 2005, we have performed EBD with limited EST for retrieval of common bile duct (CBD) stones. The patients who admitted with hyperamylasemia and gallstone pancreatitis were excluded. In cases without CBD dilation, EPBD with 12 mm for 40 seconds was performed. And in cases with CBD dilation, we dilated the sphincters with 15 mm sized balloon for 40 seconds. Total 22 patients (11 of male) were performed EBD with limited EST for retrieval of CBD stones. The median diameter of the stones was 10 mm (5-25 mm). Ten cases had multiple stones and 6 cases periampullary diverticuli. Successful stone removal in the initial session of ERCP with EBD was accomplished in 16 patients (72.7%). And complete retrieval of bile duct stones was achieved in all patients with repeated ERCP. In the aspect of complications, any episodes of perforation, bleeding was not developed. Only one case of mild grade of post-procedural pancreatitis was noted. However, post-procedural hyperamylasemia was developed in 16 cases (68.2%). EBD with larger balloon seems to be a feasible and safe alternative technique for conventional EST in CBD stone extraction.
Keyword
MeSH Terms
Figure
-
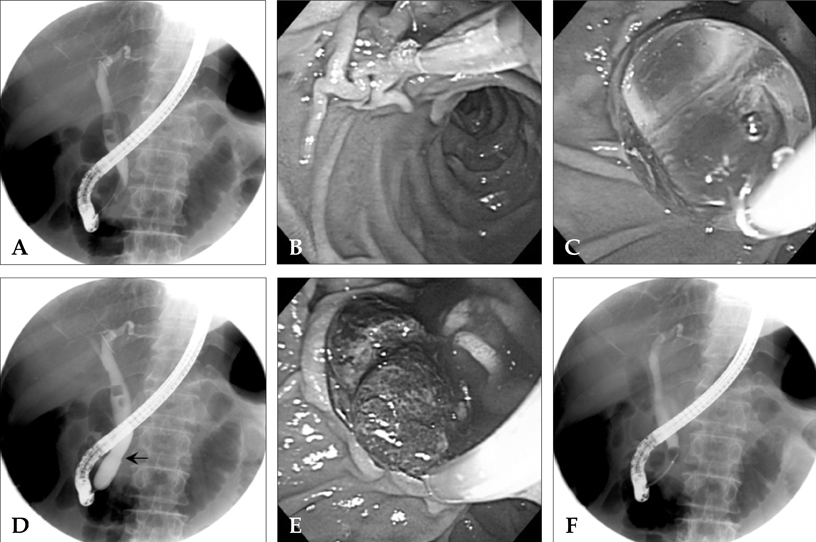
Fig. 1 Endoscopic papillary balloon dilation with limited endoscopic sphincterotomy. The endoscopic retrograde cholangiography (ERC) showed two free-floating stones, one of which was measured at 15 mm diameter, (A). A pull-type sphincterotome was inserted into the major papilla, located in the lower margin of the perivater diverticulum, (B). After limited EST, EBD with a balloon catheter of 15 mm diameter was performed, (C). The ERC showed the inflated balloon and its waist by the biliary sphincter had disappeared, black arrow, (D). With a Dormia basket, two stones were retrieved through the dilated orifice of major papilla, (E). ERC after complete stone retrieval revealed no residual filling defect in the bile duct, (F).
Reference
-
1. Classen M, Demling L. Endoscopic sphincterotomy of the papilla of vater and extraction of stones from the choledochal duct (author's transl). Dtsch Med Wochenschr. 1974. 99:496–497.2. Kawai K, Akasaka Y, Murakami K, Tada M, Koli Y. Endoscopic sphincterotomy of the ampulla of Vater. Gastrointest Endosc. 1974. 20:148–151.3. Aliperti G, Edmundowicz SA, Soper NJ, Ashley SW. Combined endoscopic sphincterotomy and laparoscopic cholecystectomy in patients with choledocholithiasis and cholecystolithiasis. Ann Intern Med. 1991. 115:783–785.4. Freeman ML. Complications of endoscopic biliary sphincterotomy: a review. Endoscopy. 1997. 29:288–297.5. Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996. 335:909–918.6. Bergman JJ, Rauws EA, Fockens P, van Berkel AM, Bossuyt PM, Tijssen JG, et al. Randomised trial of endoscopic balloon dilation versus endoscopic sphincterotomy for removal of bileduct stones. Lancet. 1997. 349:1124–1129.7. Bergman JJ, Huibregtse K. What is the current status of endoscopic balloon dilation for stone removal? Endoscopy. 1998. 30:43–45.8. Arnold JC, Benz C, Martin WR, Adamek HE, Riemann JF. Endoscopic papillary balloon dilation vs. sphincterotomy for removal of common bile duct stones: a prospective randomized pilot study. Endoscopy. 2001. 33:563–567.9. Baron TH, Harewood GC. Endoscopic balloon dilation of the biliary sphincter compared to endoscopic biliary sphincterotomy for removal of common bile duct stones during ERCP: a metaanalysis of randomized, controlled trials. Am J Gastroenterol. 2004. 99:1455–1460.10. Bergman JJ, Tytgat GN, Huibregtse K. Endoscopic dilatation of the biliary sphincter for removal of bile duct stones: an overview of current indications and limitations. Scand J Gastroenterol Suppl. 1998. 225:59–65.11. Kozarek RA. Balloon dilation of the sphincter of Oddi. Endoscopy. 1988. 20:Suppl 1. 207–210.12. Ersoz G, Tekesin O, Ozutemiz AO, Gunsar F. Biliary sphincterotomy plus dilation with a large balloon for bile duct stones that are difficult to extract. Gastrointest Endosc. 2003. 57:156–159.13. Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RC, Meyers WC, et al. Endoscopic sphincterotomy, complications and their management: an attempt at consensus. Gastrointest Endosc. 1991. 37:383–393.14. Disario JA, Freeman ML, Bjorkman DJ, Macmathuna P, Petersen BT, Jaffe PE, et al. Endoscopic balloon dilation compared with sphincterotomy for extraction of bile duct stones. Gastroenterology. 2004. 127:1291–1299.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Papillary Large Balloon Dilation: Guidelines for Pursuing Zero Mortality
- Endoscopic Papillary Balloon Dilation/Endoscopic Papillary Large Balloon Dilation
- Endoscopic Papillary Balloon Dilation for Removal of Choledocholithiasis: Indications, Advantages, Complications, and Long-Term Follow-Up Results
- Endoscopic Sphincterotomy and Endoscopic Papillary Balloon Dilation to Do It Safely
- Which Is the Better Treatment for the Removal of Large Biliary Stones? Endoscopic Papillary Large Balloon Dilation versus Endoscopic Sphincterotomy
