Coronary-Subclavian Steal Syndrome Presenting with Ventricular Tachycardia
- Affiliations
-
- 1Department of Cardiology, Gulhane Military Medical Academy, Ankara, Turkey. shurkan@superonline.com
- 2Department of Cardiology, Hacettepe University, Ankara, Turkey.
- KMID: 1777103
- DOI: http://doi.org/10.3349/ymj.2009.50.6.852
Abstract
- Coronary-subclavian steal through the left internal mammary graft is a rare cause of myocardial ischemia in patients who have had a coronary bypass surgery. We report a 70-year-old man who presented with sustained monomorphic ventricular tachycardia 5 years after the surgical creation of a left internal mammary to the left anterior descending artery. Cardiac catheterization illustrated that the left subclavian artery was occluded proximally and that the distal course was visualized by retrograde filling through the left internal mammary graft. Clinical ventricular tachycardia was reproducibly induced with a single ventricular extrastimulus, and antitachycardia pacing terminated the tachycardia. Restoration of blood flow by way of a Dacron graft placed between the descending aorta and the subclavian artery resulted in the total relief of symptoms. Ventricular tachycardia could not be induced during the control electrophysiologic study after surgical revascularization.
MeSH Terms
Figure
-
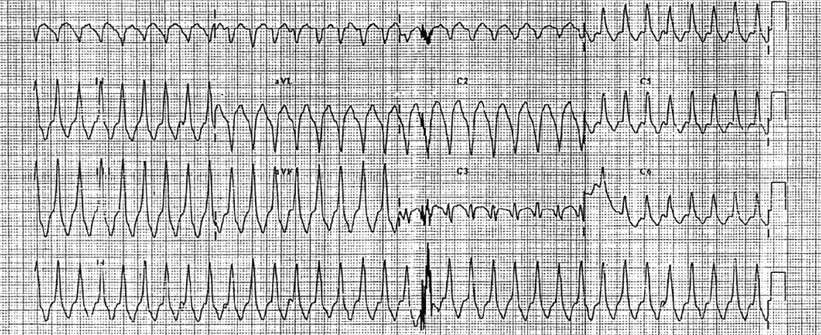
Fig. 1 Surface electrogram shows sustained monomorphic ventricular tachycardia with a left bundle branch block pattern and an inferior QRS axis.
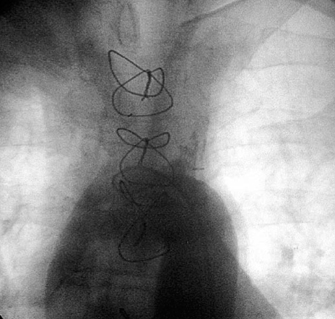
Fig. 2 Aortography shows the total occlusion from just 2 cm below of the ostium of the left subclavian artery.

Fig. 3 Left coronary angiography reveals severe stenosis of the proximal LAD and normal circumflex artery. Additionally, blood flow is observed into the LIMA from the LAD (right anterior oblique projection). LAD, left anterior descending; LIMA, left internal mammary artery.

Fig. 4 In coronary angiography because of total occlusion of left subclavian artery, the blood flow moved into the LIMA graft from the LAD, and subsequently the left subclavian artery was totally filled trough the LIMA graft. LIMA, left internal mammary artery; LAD, left anterior descending.
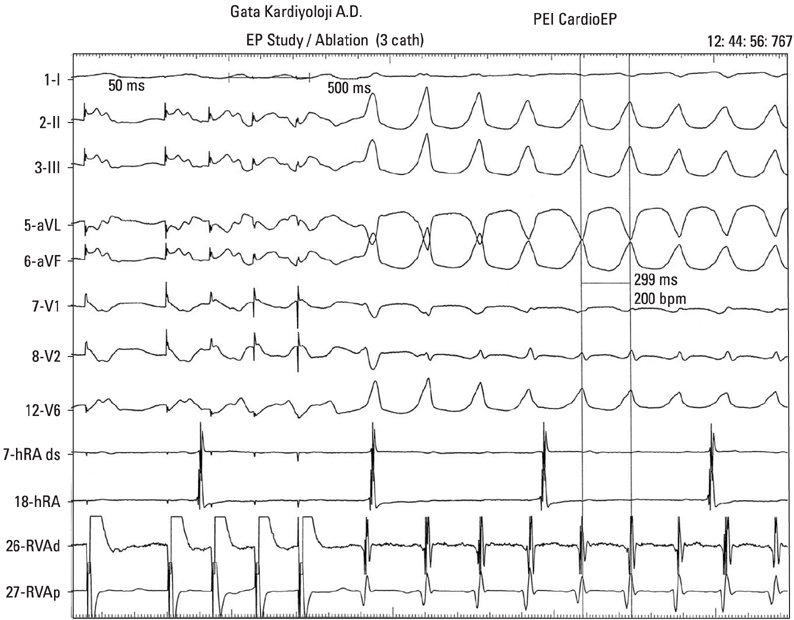
Fig. 5 After the triple extrastimulus was given to the right ventricle, It caused clinical ventricular tachycardia with left bundle branch block pattern and inferior QRS axis morphology with a cycle length of 300 msec.
Reference
-
1. Horowitz MD, Oh CJ, Jacobs JP, Chahine RA, Livingstone AS. Coronary-subclavian steal: a cause of recurrent myocardial ischemia. Ann Vasc Surg. 1993. 7:452–456.
Article2. Bryan FC, Allen RC, Lumsden AB. Coronary-subclavian steal syndrome: report of five cases. Ann Vasc Surg. 1995. 9:115–122.
Article3. Norsa A, Gamba G, Ivic N, Peranzoni P, Brunelli M, Pasquin I, et al. The coronary subclavian steal syndrome: an uncommon sequel to internal mammary-coronary artery bypass surgery. Thorac Cardiovasc Surg. 1994. 42:351–354.
Article4. Tuseth V, Hegland O, Fietland L, Nilsen DW. Reversed flow in internal mammary artery conduit and vertebral artery with left subclavian artery occlusion causing angina and vertigo. The coronary--subclavian steal syndrome. Int J Cardiol. 2001. 79:311–314.
Article5. Mary-Rabine L, Henroteaux D, Pourbaix S. [Coronary-subclavian steal syndrome: an unusual cause of recurrent myocardial ischemia following aortocoronary bypass.]. Rev Med Liege. 1994. 49:342–345.6. Rashkow AM. Angina pectoris caused by subclavian coronary steal. Cathet Cardiovasc Diagn. 1993. 30:230–232.
Article7. Philippe F, Folliguet T, Carbogniani D, Dibie A, Bouabdallah K, Larrazet F, et al. [Coronary subclavian steal syndrome after internal mammary artery bypass grafting. A cause of severe postoperative recurrent myocardial ischemia.]. Arch Mal Coeur Vaiss. 2000. 93:1555–1559.8. Nguyen NH, Reeves F, Therasse E, Latour Y, Genest J Jr. Percutaneous transluminal angioplasty in coronary-internal thoracicsubclavian steal syndrome. Can J Cardiol. 1997. 13:285–289.9. Kneale BJ, Irvine AT, Coltart DJ. Coronary subclavian steal syndrome following coronary by-pass surgery. Postgrad Med J. 1996. 72:358–360.10. Wallis F, Kidney D, Molloy M. Percutaneous transluminal angioplasty of subclavian stenosis to improve inflow to internal mammary coronary arterial grafts. Eur Radiol. 1996. 6:220–223.
Article11. Codini MA, Sommerfeldt L, Eybel CE, De Laria GA, Messer JV. Efficacy of coronary bypass grafting in exercise-induced ventricular tachycardia. J Thorac Cardiovasc Surg. 1981. 81:502–506.
Article12. Geelen P, Primo J, Wellens F, Brugada P. Coronary artery bypass grafting and defibrillator implantation in patients with ventricular tachyarrhytmias and ischemic heart disease. Pacing Clin Electrophysiol. 1999. 22:1132–1139.
Article13. Bhandari AK, Hong R, Kulick D, Petersen R, Rubin JN, Leon C, et al. Day to day reproducibility of electrically inducible ventricular arrhythmias in survivors of acute myocardial infarction. J Am Coll Cardiol. 1990. 15:1075–1081.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrence of Coronary-Subclavian Steal Syndrome After Successful Angioplasty of Malfunctioning Arteriovenous Fistula
- Axillo-axillary artery bypass graft for the treatment of subclavian steal syndrome experience of 3 cases
- A Case of Turner Syndrome with Coarctation and Subclavian Steal Syndrome by the Left Subclavian Artery from the Descending Aorta Below the Coarcted Segment
- Subclavian Steal Syndrome
- Subclavian Steal Syndrome Found Incidentally during Emergence: Difference in Blood Pressures between Both Arms: A case report
