A Case of Acute Myocardial Infarction Caused by Distal Embolization of a Left Main Coronary Artery Thrombus
- Affiliations
-
- 1Division of Cardiology, Daegu Catholic University Medical Center, Daegu, Korea. kks7379@cu.ac.kr
- KMID: 1776306
- DOI: http://doi.org/10.4070/kcj.2010.40.1.46
Abstract
- Coronary embolism is an uncommon cause of myocardial infarction. A 48-year-old male presented with typical chest pain of an MI. There was no definite ST segment change on electrocardiogram (ECG) and no elevation of myocardial enzymes. Coronary angiography (CAG) revealed occlusion of the distal left anterior descending coronary artery (dLAD), the distal left circumflex coronary artery (dLCX), the diagonal branch (D) and the obtuse marginal branch (OM), with a large filling defect in the left main coronary artery (LMA) that caused the myocardial infarction. We considered the possibility that coronary embolization was caused by the migration of a thrombus in the LMA during CAG. We did balloon angioplasty in the dLAD, dLCX, OM and D and treated the patient with glycoprotein IIb/IIIa receptor antagonist. However, thrombi remained in the dLAD, OM, and dLCX. After 3 days of anti-thrombotic treatment, follow-up CAG revealed only slight resolution of thrombi in the LAD. After triple antiplatelet agent medication for 1 year, a follow-up CAG showed a resolution of the thrombi in all coronary arteries.
Keyword
MeSH Terms
Figure
-
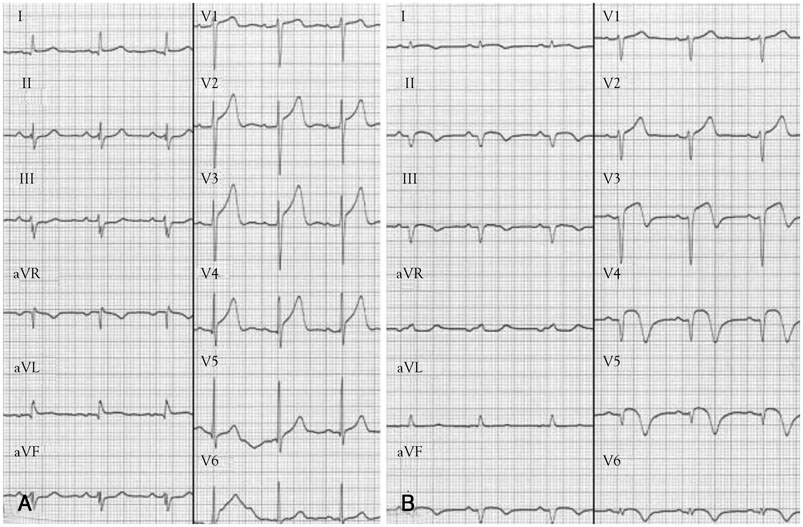
Fig. 1 ECG changes A: the initial ECG during typical chest pain shows no definite ST segment change. B: the follow-up ECG after coronary embolization shows ST segment elevation at lead II, III, aVF and V3-6. ECG: electrocardiogram. ECG changes.
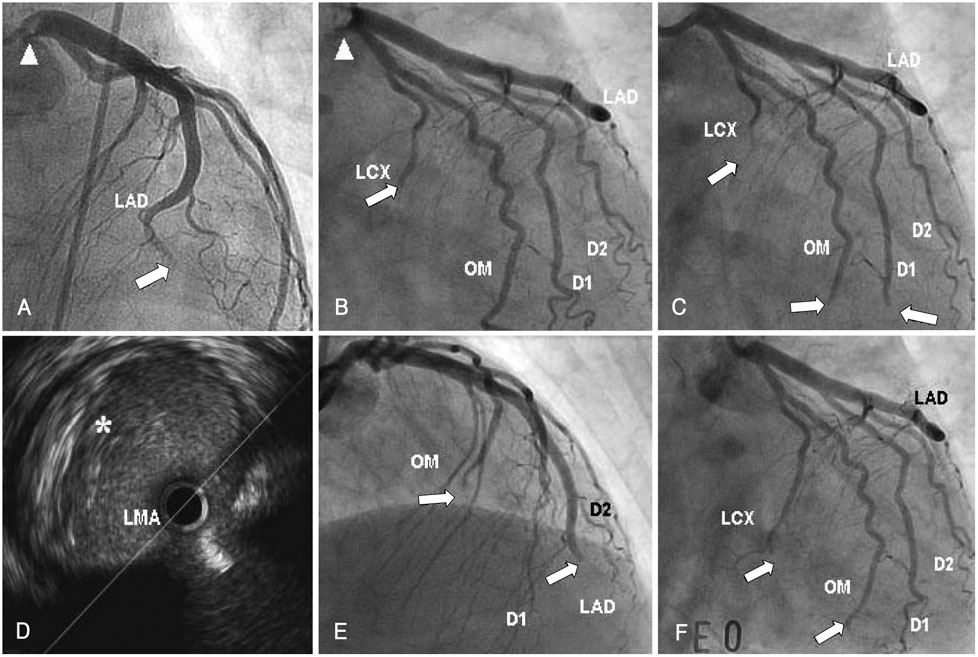
Fig. 2 The distal embolization at coronary artery. A and B: the diagnostic coronary angiogram (CAG) shows large thrombus at left main coronary artery (LMA) (arrow head) and filling defects at distal portion of left anterior descending coronary artery (LAD) and left circumflex coronary artery (LCX) (arrow). C: after engagement of guiding catheter, there are new filling defects at the obtuse marginal branch (OM) and 1st diagonal branch (D1) and larger filling defect at LCX. D: the intravascular ultrasound reveals the large thrombus at LMA (*). E and F: even though the aspiration of thrombus at LM and multiple balloonings at LAD, LCX, D1 and OM, the most of thrombi (arrow) remain except D1. A: antero-posterior cranial view, B, C and F: right anterior oblique caudal views, D: right anterior oblique cranial view.
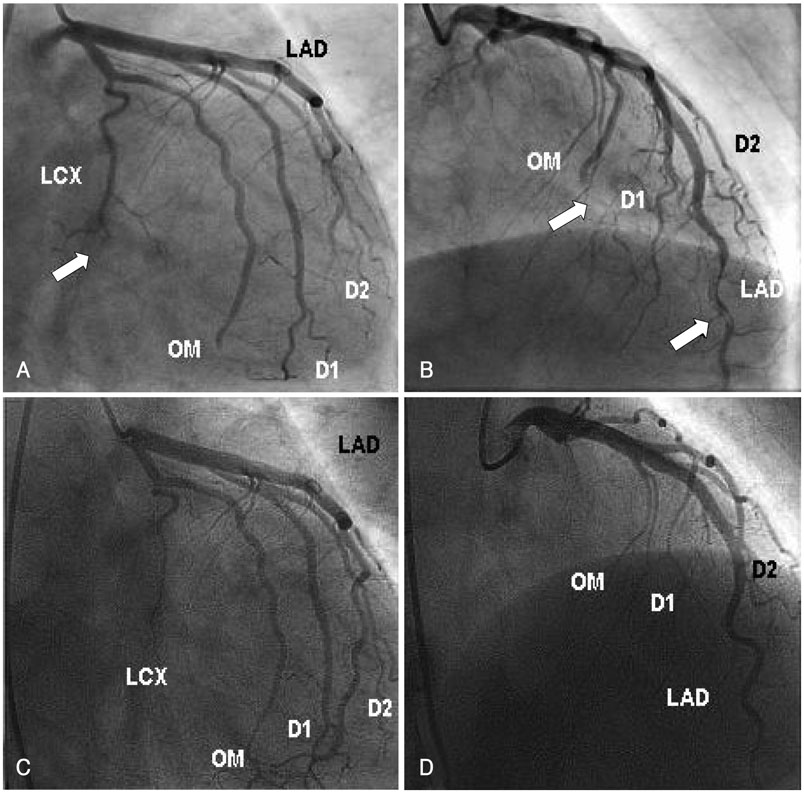
Fig. 3 Coronary angiography finding. A and B: after administration of glycoprotein IIb/IIIa receptor antagonist and intravenous unfractionated heparin for 3 days, the follow-up coronary angiography (CAG) shows slightly resolved thrombus at distal portion of the left anterior descending coronary artery (LAD) but the thrombi (arrow) at left circumflex coronary artery (LCX) and obtuse marginal branch (OM) remain. C and D: after triple antiplatelet agents for 1 year, the follow-up CAG shows no thrombus at all coronary arteries. A and C: right anterior oblique caudal views, B and D: right anterior oblique cranial views.
Reference
-
1. Kiernan TJ, Flynn AM, Kearney P. Coronary embolism causing myocardial infarction in a patient with mechanical aortic valve prosthesis. Int J Cardiol. 2006. 112:e14–e16.2. Charles RG, Epstein EJ, Holt S, Coulshod N. Coronary embolism in valvular heart disease. Q J Med. 1982. 51:147–161.3. Fuster V, Badimon L, Badimon JJ, Chesebro JH. The pathogenesis of coronary artery disease and the acute coronary syndromes (1). N Engl J Med. 1992. 326:242–250.4. Greig LD, Leslie SJ, Denvir MA. Paradoxical coronary embolism in a young woman. Int J Cardiol. 2007. 115:e17–e19.5. Belli G, Pezzano A, De Biase AM, et al. Adjunctive thrombus aspiration and mechanical protection from distal embolization in primary percutaneous intervention for acute myocardial infarction. Catheter Cardiovasc Interv. 2000. 50:362–370.6. Henriques JP, Zijlstra F, Ottervanger JP, et al. Incidence and clinical significance of distal embolization during primary angioplasty for acute myocardial infarction. Eur Heart J. 2002. 23:1112–1117.7. van Gaal WJ, West N, Banning AP. Myocardial infarction caused by distal embolisation of a ruptured left main plaque. Heart. 2006. 92:1101.8. Steinwender C, Hofmann R, Hartenthaler B, Leisch F. Resolution of a coronary embolus by intravenous application of bivalirudin. Int J Cardiol. 2009. 132:e115–e116.9. Murakami T, Mizuno S, Takahashi Y, et al. Intracoronary aspiration thrombectomy for acute myocardial infarction. Am J Cardiol. 1998. 82:839–844.10. Hajek P, Alan D, Vejvoda J, et al. Treatment of a large left main coronary artery thrombus by aspiration thrombectomy. J Thromb Thrombolysis. 2009. 27:352–354.11. Ahn SG, Tahk SJ, Whang JC, et al. Intracoronary thrombosis treated with stent and abciximab in patient with membranous glomerulonephritis. Korean Circ J. 2000. 30:1307–1311.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- No-Reflow Phoenomenon by Intracoronary Thrombus in Acute Myocardial Infarction
- A case of acute anterior and lateral myocardial infarction altering with time from a large intracoronary thrombus on left main trunk
- Detection of a Left Main Coronary Aneurysm with a Thrombus Presenting as an Acute Myocardial Infarction by Coronary Computed Tomographic Angiography
- Simultaneous Total Occlusion of Multiple Distal Coronary Arteries in Acute Myocardial Infarction
- A Case of Distal Embolization of Left Ventricular Thrombus due to Blunt Chest Trauma-Induced Coronary Artery Occlusion
