A Case of Spontaneous Coronary Artery Dissection Healed by Medical Treatment: Serial Findings of Coronary Angiography, Intravascular Ultrasound and Multi-Detector Computed Tomography
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Gyeongsang National University Hospital, Jinju, Korea. goodoctor@naver.com
- KMID: 1776195
- DOI: http://doi.org/10.4070/kcj.2011.41.6.346
Abstract
- Spontaneous coronary artery dissection (SCAD) is an uncommon cause of acute coronary syndrome which may be related to lethal condition. Although several modalities including medical therapy have been suggested, agreement on optimal treatment has not yet been determined. We describe a case of SCAD which was presented as ST-segment elevation myocardial infarction, and treated successfully with medical treatment. Coronary angiography, intravascular ultrasound and multi-detector computed tomography showed the serial changes of this disease entity.
Keyword
MeSH Terms
Figure
-
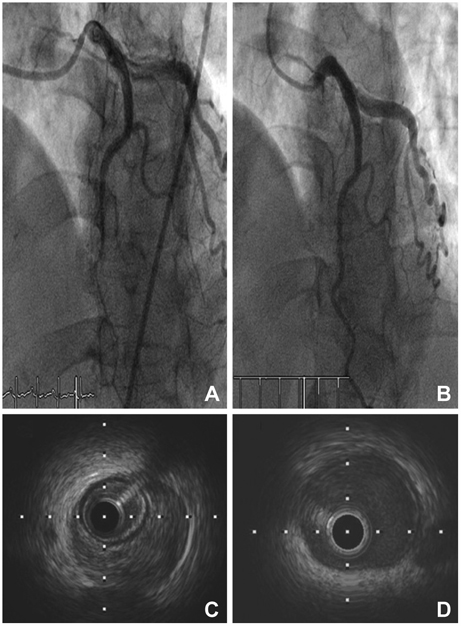
Fig. 1 Serial findings of coronary angiography (CAG) and intravascular ultrasound (IVUS) of distal left anterior descending artery (LAD). A: initial CAG showed a long and smooth lesion from the mid to distal LAD which was abruptly transitted from the proximal LAD. B: follow-up CAG revealed improved state of distal LAD. C: in the initial IVUS. The huge extramural hematoma compressing the true lumen of distal LAD. D: follow-up IVUS revealed resolved hematoma of distal LAD.
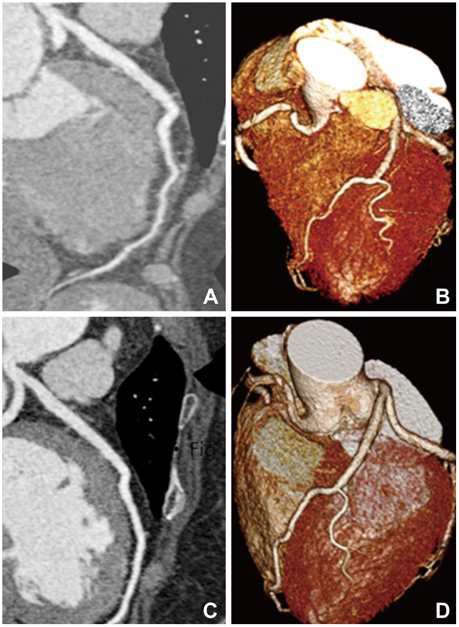
Fig. 2 Serial findings of multi-detector computed tomography (MDCT) of distal left anterior descending artery (LAD). A and B: initial MDCT manifest compressing extramural hematoma and narrowed true lumen of distal LAD. C and D: follow-up MDCT revealed disappeared hematoma and normal luminal diameter of distal LAD.
Reference
-
1. DeMaio SJ Jr, Kinsella SH, Silverman ME. Clinical course and long-term prognosis of spontaneous coronary artery dissection. Am J Cardiol. 1989. 64:471–474.2. Mortensen KH, Thuesen L, Kristensen IB, Christiansen EH. Spontaneous coronary artery dissection: a Western Denmark Heart Registry Study. Catheter Cardiovasc Interv. 2009. 74:710–717.3. Hering D, Piper C, Hohmann C, Schultheiss HP, Horstkotte D. Prospective study of the incidence, pathogenesis and therapy of spontaneous, by coronary angiography diagnosed coronary artery dissection. Z Kardiol. 1998. 87:961–970.4. Borczuk AC, van Hoeven KH, Factor SM. Review and hypothesis: the eosinophil and peripartum heart disease (myocarditis and coronary artery dissection): coincidence or pathogenetic significance? Cardiovasc Res. 1997. 33:527–532.5. Vrints CJ. Spontaneous coronary artery dissection. Heart. 2010. 96:801–808.6. Park SH, Park HS, Lee JH, et al. A case of coronary artery dissection after aortic replacement in acute type A aortic dissection. Korean Circ J. 2009. 39:428–433.7. Maehara A, Mintz GS, Castagna MT, et al. Intravascular ultrasound assessment of spontaneous coronary artery dissection. Am J Cardiol. 2002. 89:466–468.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unusual Coronary Artery Fistula: Left Anterior Descending Coronary Artery - Left Ventricular Fistula Diagnosed by ECG-Gated Multi-Detector Row Coronary CT Angiography
- Overlooked or unrecognized pitfalls in noninvasive multi-detector computed tomography coronary angiography
- Spontaneous Coronary Artery Dissection and Woven Coronary Artery: Three Cases and a Review of the Literature
- Two Cases of Spontaneous Coronary Artery Dissection
- Spontaneous Coronary Artery Dissection in a female patient with fragile X syndrome
