Korean Circ J.
2011 Jun;41(6):308-312. 10.4070/kcj.2011.41.6.308.
The Impact of Moderate to Severe Renal Insufficiency on Patients With Acute Myocardial Infarction
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Keimyung University, Daegu, Korea. shur@dsmc.or.kr
- KMID: 1776187
- DOI: http://doi.org/10.4070/kcj.2011.41.6.308
Abstract
- BACKGROUND AND OBJECTIVES
Renal insufficiency (RI) has been reported to be associated with unfavorable clinical outcomes in patients undergoing percutaneous coronary interventions (PCI). However, little data is available regarding the impact of moderate to severe RI on clinical outcomes in patients with acute myocardial infarction (AMI) undergoing PCI.
SUBJECTS AND METHODS
Between March 2003 and July 2007, 878 patients with AMI who underwent PCI were enrolled. Based on estimated glomerular filtration rate (eGFR) using the Modification of Diet in Renal Disease (MDRD) equation, patients were divided into two groups: eGFR <60 mL/min.m2 (moderate to severe RI, group A) and eGFR > or =60 mL/min.m2 (normal to mild RI, group B). The primary endpoint was all-cause mortality at 1-year after successful PCI. The secondary endpoints were non-fatal myocardial infarction (MI), target lesion revascularization (TLR), target vessel revascularization (TVR), stent thrombosis (ST) and major adverse cardiac events (MACE) at 1-year.
RESULTS
In group A, patients were more often male and older, with diabetes and hypertension. Compared to patients in group B, group A showed significantly higher incidences of all-cause mortality, cardiac mortality, non-fatal MI and MACE. The needs of TLR and TVR, and the incidence of ST were not significantly different between the two groups. Independent predictors of 1-year mortality were eGFR <60 mL/min.m2, male gender, older age and a lower left ventricular ejection fraction.
CONCLUSION
In patients with AMI, moderate to severe RI was associated with mortality and MACE at 1-year after successful PCI. In addition, eGFR <60 mL/min.m2 was a strong independent predictor of 1-year mortality.
MeSH Terms
Figure
-
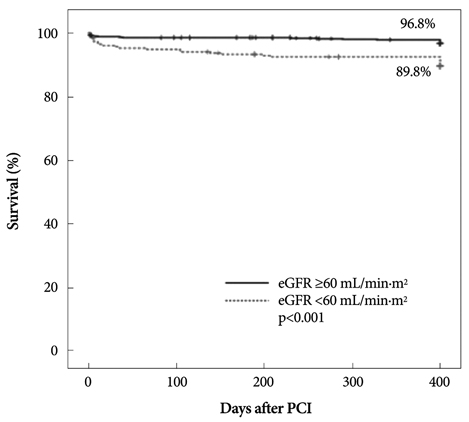
Fig. 1 Kaplan-Meier survival according to renal insufficiency.
Reference
-
1. Best PJ, Lennon R, Ting HH, et al. The impact of renal insufficiency on clinical outcomes in patients undergoing percutaneous coronary interventions. J Am Coll Cardiol. 2002. 39:1113–1119.2. Singh M, Rihal CS, Selzer F, Kip KE, Detre K, Holmes DR. Validation of Mayo Clinic risk adjustment model for in-hospital complications after percutaneous coronary interventions, using the National Heart, Lung, and Blood Institute dynamic registry. J Am Coll Cardiol. 2003. 42:1722–1728.3. Feldman DN, Gade CL, Slotwiner AJ, et al. Comparison of outcomes of percutaneous coronary interventions in patients of three age groups (<60, 60 to 80, and >80 years) (from the New York State Angioplasty Registry). Am J Cardiol. 2006. 98:1334–1339.4. Gruberg L, Dangas G, Mehran R, et al. Clinical outcome following percutaneous coronary interventions in patients with chronic renal failure. Catheter Cardiovasc Interv. 2002. 55:66–72.5. Klein LW, Block P, Brindis RG, et al. Percutaneous coronary interventions in octogenarians in the American College of Cardiology-National Cardiovascular Data Registry: development of a nomogram predictive of in-hospital mortality. J Am Coll Cardiol. 2002. 40:394–402.6. Beattie JN, Soman SS, Sandberg KR, et al. Determinants of mortality after myocardial infarction in patients with advanced renal dysfunction. Am J Kidney Dis. 2001. 37:1191–1200.7. Zhang RY, Zhu ZB, Zhang Q, et al. Impact of moderate or severe renal insufficiency on long-term outcomes in patients undergoing drug-eluting stent based coronary intervention. Int J Cardiol. 2009. 136:72–79.8. Yamaguchi J, Kasanuki H, Ishii Y, et al. Prognostic significance of se-rum creatinine concentration for in-hospital mortality in patients with acute myocardial infarction who underwent successful primary percutaneous coronary intervention (from the Heart Institute of Japan Acute Myocardial Infarction [HIJAMI] Registry). Am J Cardiol. 2004. 93:1526–1528.9. Kidney National Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002. 39:2 Suppl 1. S1–S266.10. Shlipak MG, Heidenreich PA, Noguchi H, Chertow GM, Browner WS, McClellan MB. Association of renal insufficiency with treatment and outcomes after myocardial infarction in elderly patients. Ann Intern Med. 2002. 137:555–562.11. Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007. 115:2344–2351.12. Hsu CY, Iribarren C, McCulloch CE, Darbinian J, Go AS. Risk factors for end-stage renal disease: 25-year follow-up. Arch Intern Med. 2009. 169:342–350.13. Plantinga LC, Boulware LE, Coresh J, et al. Patient awareness of chronic kidney disease: trends and predictors. Arch Intern Med. 2008. 168:2268–2275.14. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. Modification of Diet in Renal Disease Study Group. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med. 1999. 130:461–470.15. Kanani PM, Sinkey CA, Browning RL, Allaman M, Knapp HR, Haynes WG. Role of oxidant stress in endothelial dysfunction produced by experimental hyperhomocyst(e)inemia in humans. Circulation. 1999. 100:1161–1168.16. Massy ZA, Kasiske BL. Hyperlipidemia and its management in renal disease. Curr Opin Nephrol Hypertens. 1996. 5:141–146.17. Romanic AM, Arleth AJ, Willette RN, Ohlstein EH. Factor XIIIa cross-links lipoprotein(a) with fibrinogen and is present in human atherosclerotic lesions. Circ Res. 1998. 83:264–269.18. Busch M, Franke S, Muller A, et al. Potential cardiovascular risk factors in chronic kidney disease: AGEs, total homocysteine and metabolites, and the C-reactive protein. Kidney Int. 2004. 66:338–347.19. Bjorkbacka H, Kunjathoor VV, Moore KJ, et al. Reduced atherosclerosis in MyD88-null mice links elevated serum cholesterol levels to activation of innate immunity signaling pathways. Nat Med. 2004. 10:416–421.20. Cheung AK, Sarnak MJ, Yan G, et al. Atherosclerotic cardiovascular disease risks in chronic hemodialysis patients. Kidney Int. 2000. 58:353–362.21. Choi JH, Kim KL, Huh W, et al. Decreased number and impaired angiogenic function of endothelial progenitor cells in patients with ch-ronic renal failure. Arterioscler Thromb Vasc Biol. 2004. 24:1246–1252.22. Herzog CA, Ma JZ, Collins AJ. Poor long-term survival after acute myocardial infarction among patients on long-term dialysis. N Engl J Med. 1998. 339:799–805.23. Chertow GM, Normand SL, Silva LR, McNeil BJ. Survival after acute myocardial infarction in patients with end-stage renal disease: results from the cooperative cardiovascular project. Am J Kidney Dis. 2000. 35:1044–1051.24. Wright RS, Reeder GS, Herzog CA, et al. Acute myocardial infarction and renal dysfunction: a high-risk combination. Ann Intern Med. 2002. 137:563–570.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Invasive Treatment of Acute Myocardial Infarction: What is the Optimal Therapy for Acute Myocardial Infarction?
- Primary Coronary Stenting as a Successful Treatment of Acute Myocardial
- A Case of Pericardial Effusion after Acute Myocardial Infarction
- The simpler, the better: culprit-only intervention is beneficial in patients with chronic kidney disease with concurrent acute myocardial infarction and multivessel disease
- Impact of Acute Kidney Injury on Clinical Outcomes after ST Elevation Acute Myocardial Infarction
