Small Cell Carcinoma of Extahepatic Bile Duct Presenting with Hemobilia
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea. yejoo@chonnam.ac.kr
- KMID: 1775956
- DOI: http://doi.org/10.4166/kjg.2009.54.3.186
Abstract
- We report a case of small cell carcinoma of extrahepatic bile duct presenting with jaundice and hemobilia. A 59-year-old woman was admitted due to right upper quadrant pain and jaundice. An abdominal computed tomography revealed a 2 cm sized mass in the extrahepatic bile duct. Endoscopic retrograde cholangiopancreatography revealed bloody discharge coming out of the papillary orifice in endoscopic view and a dilated extrahepatic bile duct with multiple irregular filling defects in cholangiogram. A coronal T2-weighted image revealed a hyperintense mass at extrahepatic bile duct. Laparotomy was performed, and pathologic examination of resected specimen showed tumor cells having round to oval nuclei with coarsely granular chromatin and scanty cytoplasm, which were immunoreactive for synaptophysin and chromogranin A, compatible with the diagnosis of small cell carcinoma. The small cell carcinoma of bile duct, despite its rarity, should be considered in differential diagnosis of the causes for obstructive jaundice and hemobilia.
Keyword
MeSH Terms
-
Bile Duct Neoplasms/*diagnosis/pathology/radiography
Bile Ducts, Extrahepatic/*pathology/radiography
Carcinoma, Small Cell/*diagnosis/pathology/radiography
Cholangiopancreatography, Endoscopic Retrograde
Chromogranin A/metabolism
Female
Hemobilia/complications/*diagnosis
Humans
Magnetic Resonance Imaging
Middle Aged
Synaptophysin/metabolism
Tomography, X-Ray Computed
Figure
-
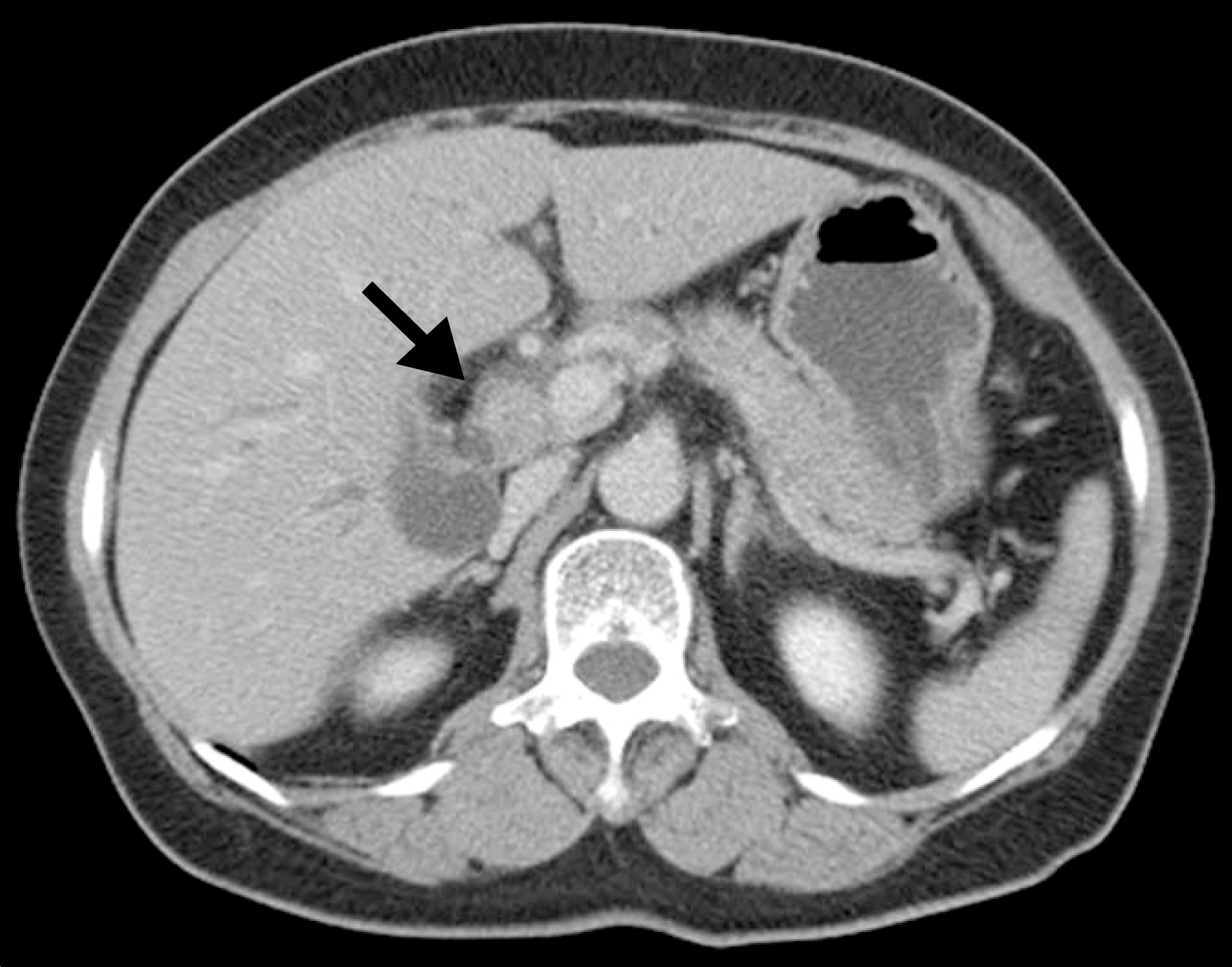
Fig. 1. An abdominal computed tomography revealed a 2 cm sized enhancing mass (arrow) in the extrahepatic bile duct.
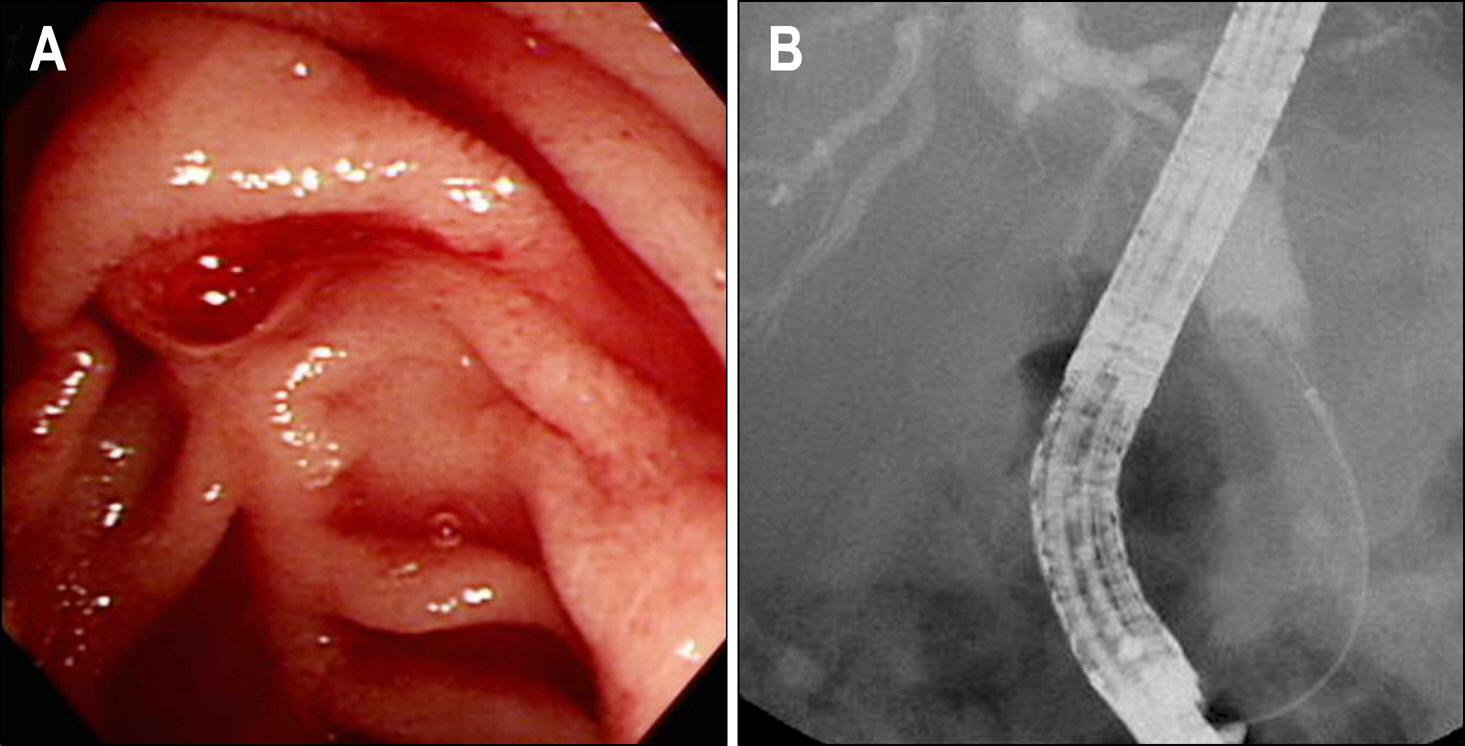
Fig. 2. Endoscopic retrograde cholangiopancreatographic findings. (A) It revealed bloody discharge coming out from the papillary orifice. (B) It showed a dilated bile duct with multiple irregular filling defects.

Fig. 3. A coronal T2-weighted image of magnetic resonance revealed an exophytic intermediate hyperintense mass (arrow) in the extrahepatic bile duct.
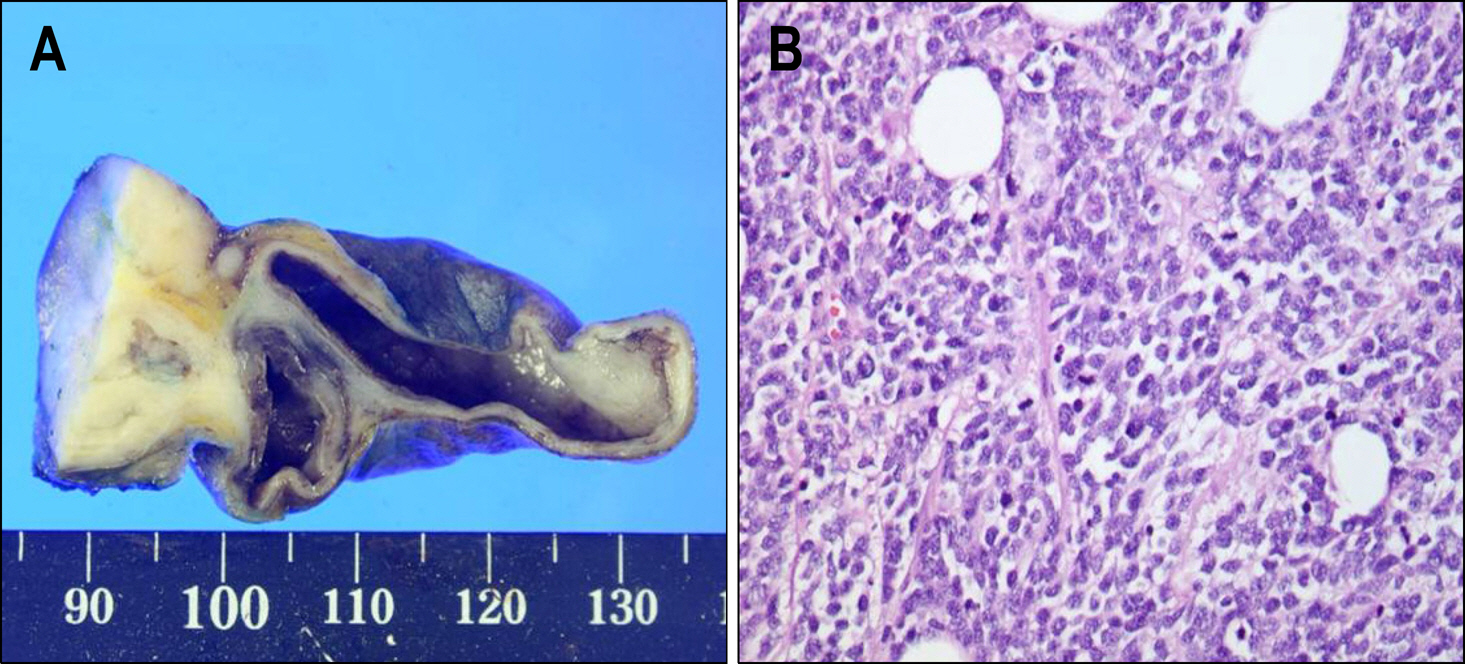
Fig. 4. Pathologic findings of resected specimen. (A) Gross specimen showed a hard tumor measuring 3.0×3.0 cm located in extrahepatic bile duct. (B) Pathologic examination of resected specimen, stained using hematoxylin-eosin showed tumor cells having round to oval nuclei with coarsely granular chromatin and scanty cytoplasm (H&E stain, ×400).
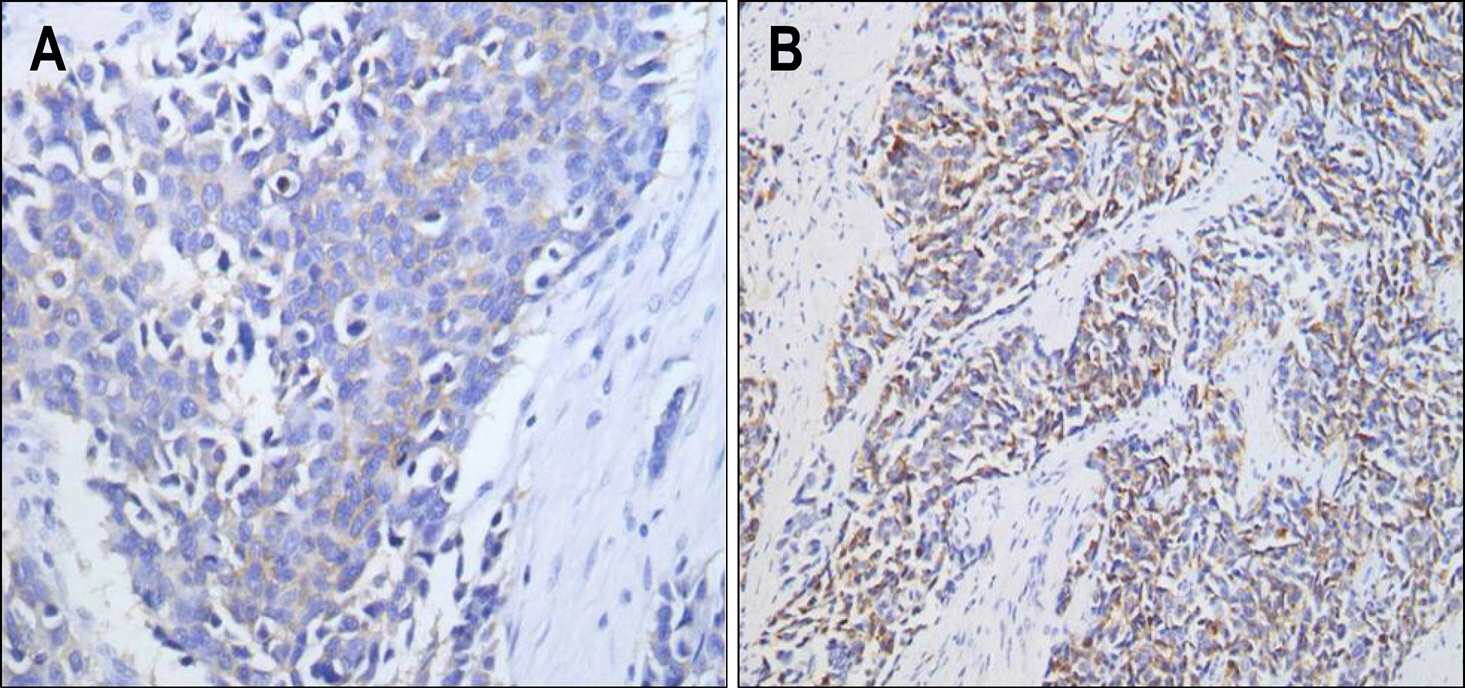
Fig. 5. In immunohistochemical staining, neuroendocrine cell marker, synaptophysin (A) and chromogranin A (B) were strongly positive.
Reference
-
1. Chamberlain RS, Blumgart LH. Carcinoid tumors of the extrahepatic bile duct. A rare cause of malignant biliary obstruction. Cancer. 1999; 86:1959–1965.2. Fenoglio-Preiser CM. Gastrointestinal neuroendocrine/neuro-ectodermal tumors. Am J Clin Pathol. 2001; 115(suppl):S79–S93.
Article3. Carriaga MT, Henson DE. Liver, gallbladder, extrahepatic bile ducts, and pancreas. Cancer. 1995; 75:171–190.
Article4. Levenson RM Jr, Ihde DC, Matthews MJ, et al. Small cell carcinoma presenting as an extrapulmonary neoplasm: sites of origin and response to chemotherapy. J Natl Cancer Inst. 1981; 67:607–612.5. Green MH, Duell RM, Johnson CD, Jamieson NV. Haemo-bilia. Br J Surg. 2001; 88:773–786.
Article6. Yoshida J, Donahue PE, Nyhus LM. Hemobilia: review of recent experience with a worldwide problem. Am J Gastroenterol. 1987; 82:448–453.7. Travis WD, Rush W, Flieder DB, et al. Survival analysis of 200 pulmonary neuroendocrine tumors with clarification of criteria for atypical carcinoid and its separation from typical carcinoid. Am J Surg Pathol. 1998; 22:934–944.
Article8. Sabanathan S, Hashimi H, Nicholson G, Edwards AS. Primary oat cell carcinoma of the common bile duct. J R Coll Surg Edinb. 1988; 33:285–286.9. van der Wal AC, Van Leeuwen DJ, Walforld N. Small cell neuroendocrine (oat cell) tumour of the common bile duct. Histopathology. 1990; 16:398–400.
Article10. Nishihara K, Tsuneyoshi M, Niiyama H, Ichimiya H. Composite glandular-endocrine cell carcinoma of the extrahepatic bile duct: Immunohistochemical study. Pathology. 1993; 25:90–94.
Article11. Kim SH, Park YN, Yoon DS, Lee SJ, Yu JS, Noh TW. Composite neuroendocrine and adenocarcinoma of the common bile duct associated with Clonorchis sinensis. A case report. Hepatogastroenterology. 2000; 47:942–944.12. Hazama K, Suzuki Y, Takahashi M, et al. Primary small cell carcinoma of the common bile duct, in which surgical treatment was performed after neoaduvant chemotherapy: report of a case. Surg Today. 2003; 33:870–872.13. Kuraoka K, Taniyama K, Fujitaka T, Nakatsuka H, Nakayama H, Yasui W. Small cell carcinoma of the extrahepatic bile duct: case report and immunohistochemical analysis. Pathol Int. 2003; 53:887–891.
Article14. Kim SH, Park YN, Yoon DS, Lee SJ, Yu JS, Noh TW. Extrapulmonary small-cell carcinoma: a single-institution experience. Jpn J Clin Oncol. 2004; 34:250–254.
Article15. Thomas NE, Burroughs FH, Ali SZ. Small-cell carcinoma of the extrahepatic bile duct and concurrent clonorchiasis. Diagn Cytopathol. 2005; 32:92–93.
Article16. Kaiho T, Tanaka T, Tsuchiya S, et al. A case of small cell carcinoma of the common bile duct. Hepatogastroenterology. 2005; 52:363–367.17. Arakura N, Muraki T, Komatsu K, et al. Small cell carcinoma of the extrahepatic bile duct diagnosed with EUS-FNA and effectively treated with chemoradiation. Intern Med. 2008; 47:621–625.
Article18. Jeon WJ, Chae HB, Park SM, Youn SJ, Choi JW, Kim SH. A case of primary small cell carcinoma arising from the common bile duct. Korean J Gastroenterol. 2006; 48:438–442.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hepatoma presenting as extrahepatic biliary obstruction due to hemobilia
- Common Bile Duct Obstruction Caused by Tumor Thrombus after Trans-arterial Chemoembolization in a Hepatocellular Carcinoma Patient
- Two Cases of Hemobilia Associated with Common Bile Duct Stones
- Delayed Severe Hemobilia after Endoscopic Biliary Plastic Stent Insertion
- A Case of Primary Small Cell Carcinoma in the Common Bile Duct
