Korean J Gastroenterol.
2013 Apr;61(4):230-233. 10.4166/kjg.2013.61.4.230.
A Case of Angiographic Embolization of Aortoenteric Fistula Caused by Endovascular Stent Grafting for an Abdominal Aortic Aneurysm
- Affiliations
-
- 1Department of Internal Medicine, Chungnam National University School of Medicine, Daejeon, Korea. mhs1357@hanmail.net
- KMID: 1775764
- DOI: http://doi.org/10.4166/kjg.2013.61.4.230
Abstract
- Aortoenteric fistula (AEF) developed after treatment for an abdominal aortic aneurysm (AAA) is a rare but usually fatal complication. We report a rare case of AEF bleeding after endovascular stent grafting for AAA which was managed angiographically. An 81-year-old man presented with hematochezia and acute abdominal pain for 1 day ago. Four years ago, an aortic stent was implanted in the infrarenal aorta for AAA. Endoscopies were performed to evaluate the hematochezia. Evidence of gastrointestinal bleeding was observed, but a clear bleeding point was not detected on upper endoscopy and colonoscopy. Contrast-enhanced computed tomography performed subsequently showed that the bleeding point was located in the fourth portion of the duodenum as an AEF caused by an inflammatory process in the stent-graft. Intra-arterial angiography showed a massive contrast leakage into the bowel via a small fistula from around the aortic stent graft site. Embolization was successfully performed by injecting a mixture of glue and lipiodol into the AEF tract. The patient was discharged with no evidence of gastrointestinal bleeding after the embolization.
MeSH Terms
Figure
-
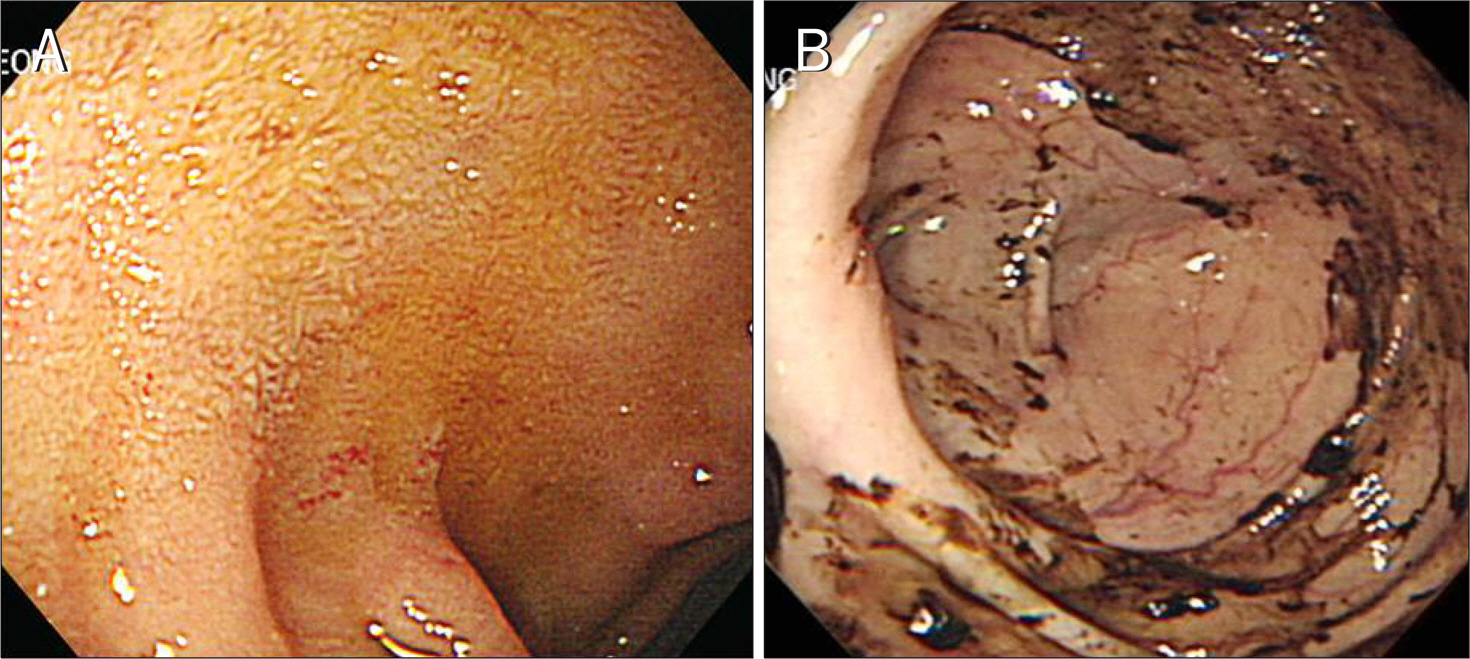
Fig. 1. (A) Duodenoscopy showing no evidence of a bleeding focus. (B) Melena was detected by colonoscopy, suggesting bleeding in the upper intestinal tract.

Fig. 2. (A) Computed tomography scan showing a bleeding point in the fourth portion of the duodenum, suggesting an aortoenteric fistula (arrow). (B) Computed tomography scan showing a small foci of air around the frame of the device (arrow head).

Fig. 3. Angiography showing contrast leakage into the bowel via the fistula tract.
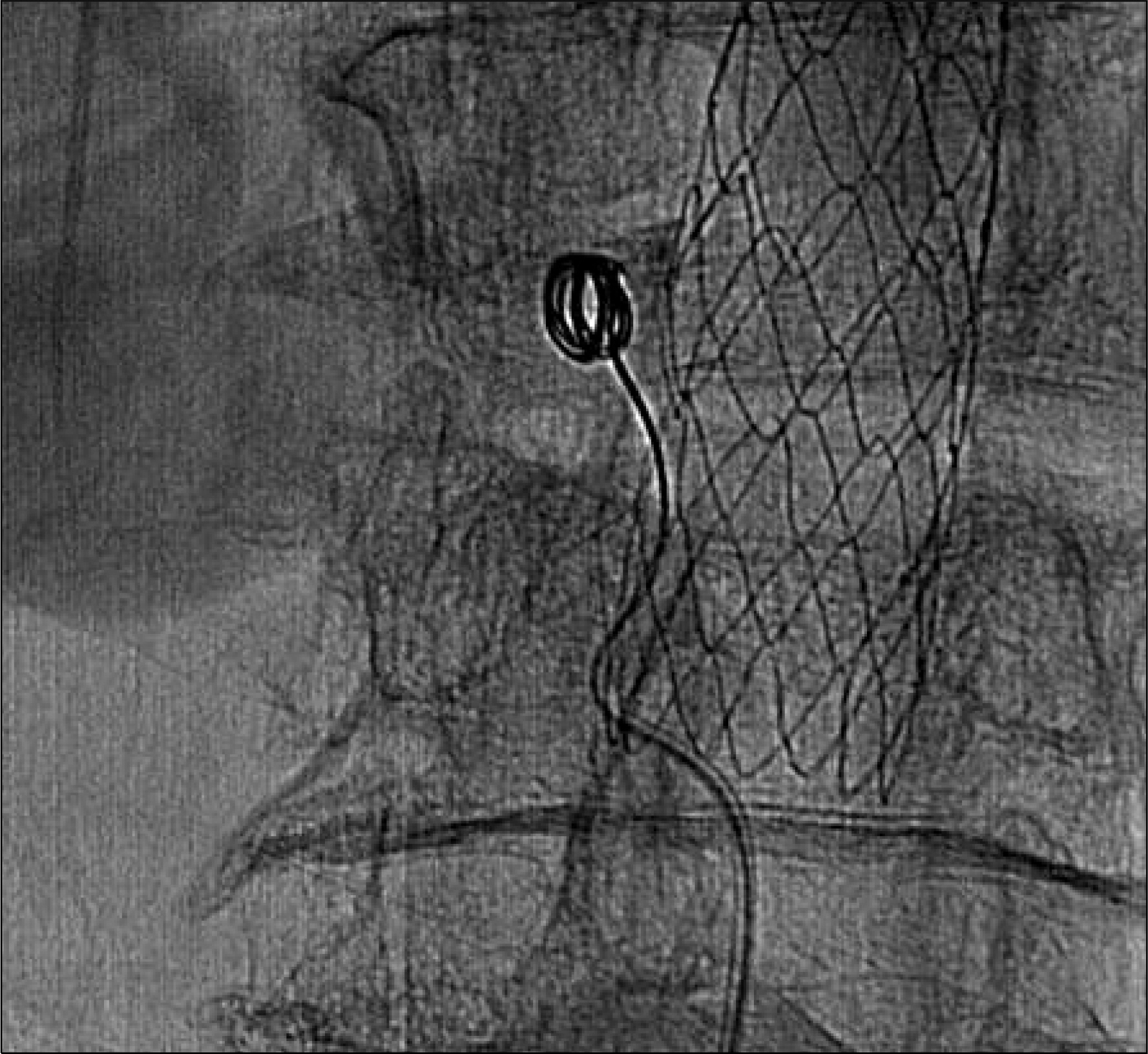
Fig. 4. Microcoils were inserted into sac-like dilatation of the fistula tract.

Fig. 5. Embolization was performed by injecting a mixture of glue and lipiodol. After the procedure there was no longer any leakage of contrast through the fistula tract.
Reference
-
References
1. Flye MW, Thompson WM. Aortic graft-enteric and para-prosthetic-enteric fistulas. Am J Surg. 1983; 146:183–187.
Article2. Voorhoeve R, Moll FL, de Letter JA, Bast TJ, Wester JP, Slee PH. Primary aortoenteric fistula: report of eight new cases and review of the literature. Ann Vasc Surg. 1996; 10:40–48.
Article3. Reynolds JV, Galloway JM. Primary aortoduodenal fistula: a case report and review of the literature. Ir J Med Sci. 1991; 160:381–384.
Article4. Brock RC. Aortic homografting; a report of six successful cases. Guys Hosp Rep. 1953; 102:204–228.5. Birch L, Cardwell ES, Claytor H, Zimmerman SL. Suture-line rupture of a nylon aortic bifurcation graft into the small bowel. AMA Arch Surg. 1956; 73:947–950.6. Yu SB, Park SC, Moon IS, Koh YB. Primary aortoduodenal fistula in salmonella mycotic aortic aneurysm: a case report. J Korean Soc Vasc Surg. 2003; 19:79–82.7. Kalman DR, Barnard GF, Massimi GJ, Swanson RS. Primary aortoduodenal fistula after radiotherapy. Am J Gastroenterol. 1995; 90:1148–1150.8. Broadbent NR, Taylor DE. Gallstone erosion of the aorta. Aust N Z J Surg. 1975; 45:207–208.
Article9. Saers SJ, Scheltinga MR. Primary aortoenteric fistula. Br J Surg. 2005; 92:143–152.
Article10. Berry SM, Fischer JE. Classification and pathophysiology of enterocutaneous fistulas. Surg Clin North Am. 1996; 76:1009–1018.
Article11. Sweeney MS, Gadacz TR. Primary aortoduodenal fistula: manifestation, diagnosis, and treatment. Surgery. 1984; 96:492–497.12. Elliott JP Jr, Smith RF, Szilagyi DE. Proceedings: Aortoenteric and paraprosthetic-enteric fistulas. Problems of diagnosis and management. Arch Surg. 1974; 108:479–490.13. Korkut AK, Arpinar E, Yasar T, Guney D. Primary aortoduodenal fistula complicated by abdominal aortic aneurysm. J Cardiovasc Surg (Torino). 2000; 41:113–115.14. Mylona S, Ntai S, Pomoni M, Kokkinaki A, Lepida N, Thanos L. Aortoenteric fistula: CT findings. Abdom Imaging. 2007; 32:393–397.
Article15. Brand EJ, Sivak MV Jr, Sullivan BH Jr. Aortoduodenal fistula: endoscopic diagnosis. Dig Dis Sci. 1979; 24:940–944.16. Kim JY, Kim YW, Kim CJ, Lim HI, Kim DI, Huh S. Successful surgical treatment of aortoenteric fisula. J Korean Med Sci. 2007; 22:846–850.17. Loftus IM, Thompson MM, Fishwick G, et al. Technique for rapid control of bleeding from an aortoenteric fistula. Br J Surg. 1997; 84:1114.
Article18. Karkos CD, Bruce IA, Lambert ME. Use of the intra-aortic balloon pump to arrest gastrointestinal bleeding. Ann Emerg Med. 2001; 38:328–331.19. Finch L, Heathcock RB, Quigley T, et al. Emergent treatment of a primary aortoenteric fistula with N-butyl 2-cyanoacrylate and endovascular stent. J Vasc Interv Radiol. 2002; 13:841–843.
Article20. Cekirge S, Oguzkurt L, Saatci I, et al. Embolization of a high-out-put post-nephrectomy aortocaval fistula with Gianturco coils and cyanoacrylate. Cardiovasc Intervent Radiol. 1996; 19:56–58.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary Aortoenteric Fistula of a Saccular Aneurysm: Case Study and Literature Review
- A case of aortoduodenal fistula and vertebral erosion caused by an abdominal aortic aneurysm
- Unusual Perigraft Abscess Formation Associated with Stent Graft Infection after Endovascular Aortic Repair of Abdominal Aortic Aneurysm: A Case Report
- Aorto-Uni-Iliac Stent Grafting and Femoro-Femoral Bypass in a Patient with a Failed and Catastrophic Endovascular Aortic Aneurysm Repair
- Stented Aortic Graft Insertion in an Infrarenal Abdominal Aortic Aneurysm as Performed by Cardiovascular Surgeons: Report of 3 cases
